

Severe mental illness and health service utilisation for nonpsychiatric medical disorders: A systematic review and meta-analysis
- PMID: 32925912
- PMCID: PMC7489517
- DOI: 10.1371/journal.pmed.1003284
Severe mental illness and health service utilisation for nonpsychiatric medical disorders: A systematic review and meta-analysis
Abstract
Background: Psychiatric comorbidity is known to impact upon use of nonpsychiatric health services. The aim of this systematic review and meta-analysis was to assess the specific impact of severe mental illness (SMI) on the use of inpatient, emergency, and primary care services for nonpsychiatric medical disorders.
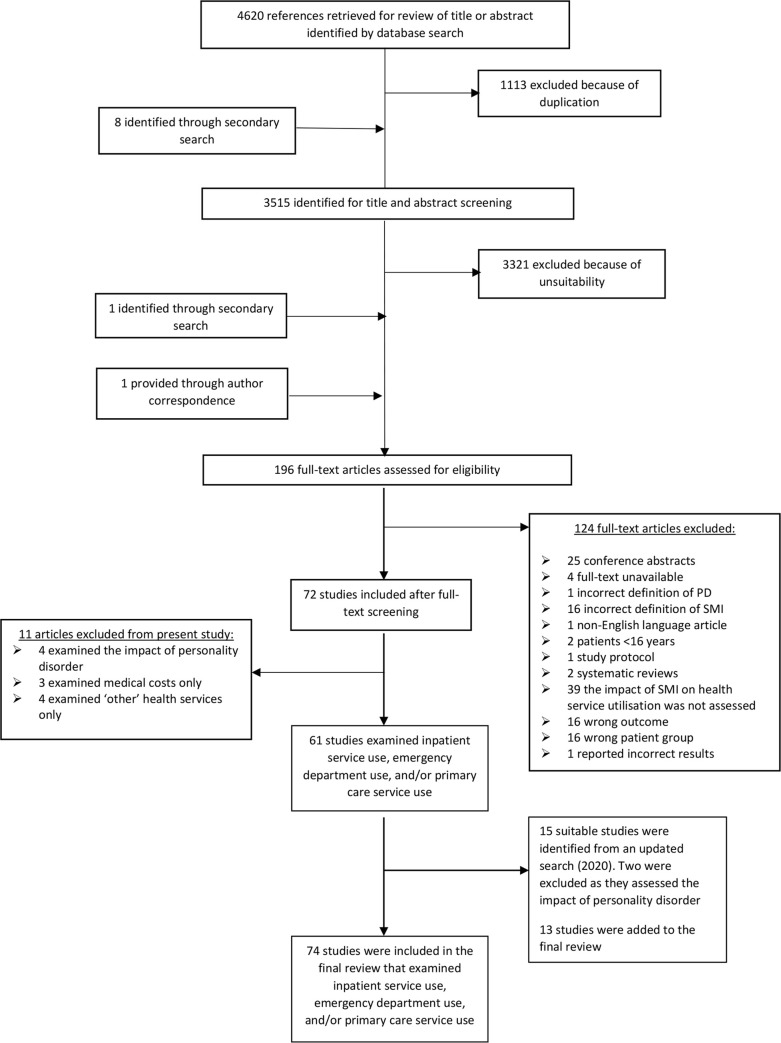
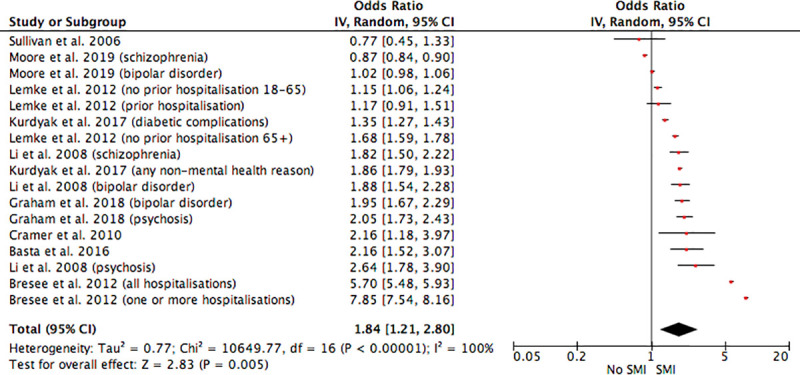
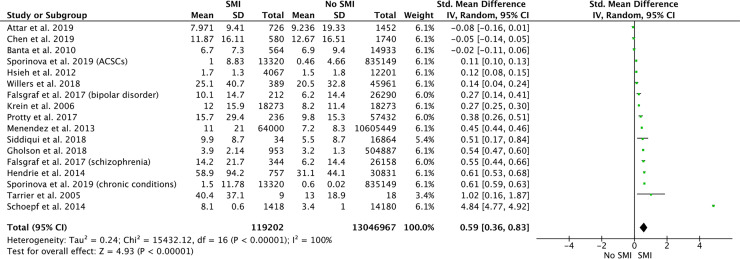
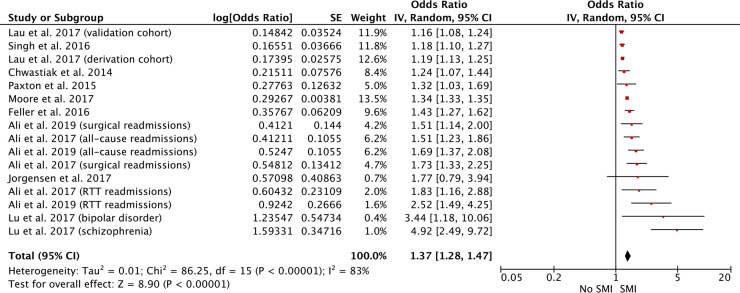
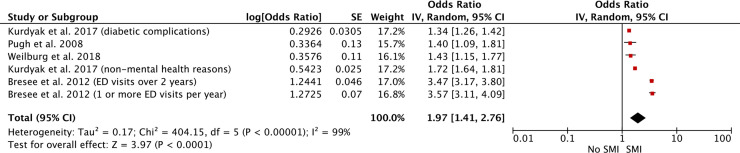
Methods and findings: PubMed, Web of Science, PsychINFO, EMBASE, and The Cochrane Library were searched for relevant studies up to October 2018. An updated search was carried out up to the end of February 2020. Studies were included if they assessed the impact of SMI on nonpsychiatric inpatient, emergency, and primary care service use in adults. Study designs eligible for review included observational cohort and case-control studies and randomised controlled trials. Random-effects meta-analyses of the effect of SMI on inpatient admissions, length of hospital stay, 30-day hospital readmission rates, and emergency department use were performed. This review protocol is registered in PROSPERO (CRD42019119516). Seventy-four studies were eligible for review. All were observational cohort or case-control studies carried out in high-income countries. Sample sizes ranged from 27 to 10,777,210. Study quality was assessed using the Newcastle-Ottawa Scale for observational studies. The majority of studies (n = 45) were deemed to be of good quality. Narrative analysis showed that SMI led to increases in use of inpatient, emergency, and primary care services. Meta-analyses revealed that patients with SMI were more likely to be admitted as nonpsychiatric inpatients (pooled odds ratio [OR] = 1.84, 95% confidence interval [CI] 1.21-2.80, p = 0.005, I2 = 100%), had hospital stays that were increased by 0.59 days (pooled standardised mean difference = 0.59 days, 95% CI 0.36-0.83, p < 0.001, I2 = 100%), were more likely to be readmitted to hospital within 30 days (pooled OR = 1.37, 95% CI 1.28-1.47, p < 0.001, I2 = 83%), and were more likely to attend the emergency department (pooled OR = 1.97, 95% CI 1.41-2.76, p < 0.001, I2 = 99%) compared to patients without SMI. Study limitations include considerable heterogeneity across studies, meaning that results of meta-analyses should be interpreted with caution, and the fact that it was not always possible to determine whether service use outcomes definitively excluded mental health treatment.
Conclusions: In this study, we found that SMI impacts significantly upon the use of nonpsychiatric health services. Illustrating and quantifying this helps to build a case for and guide the delivery of system-wide integration of mental and physical health services.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Comment in
-
Research round up.Lancet Psychiatry. 2020 Nov;7(11):937. doi: 10.1016/S2215-0366(20)30439-9. Lancet Psychiatry. 2020. PMID: 33069312 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
