

Temporal Dysbiosis of Infant Nasal Microbiota Relative to Respiratory Syncytial Virus Infection
- PMID: 32926147
- PMCID: PMC8136976
- DOI: 10.1093/infdis/jiaa577
Temporal Dysbiosis of Infant Nasal Microbiota Relative to Respiratory Syncytial Virus Infection
Abstract
Background: Respiratory syncytial virus (RSV) is a leading cause of infant respiratory disease. Infant airway microbiota has been associated with respiratory disease risk and severity. The extent to which interactions between RSV and microbiota occur in the airway, and their impact on respiratory disease susceptibility and severity, are unknown.
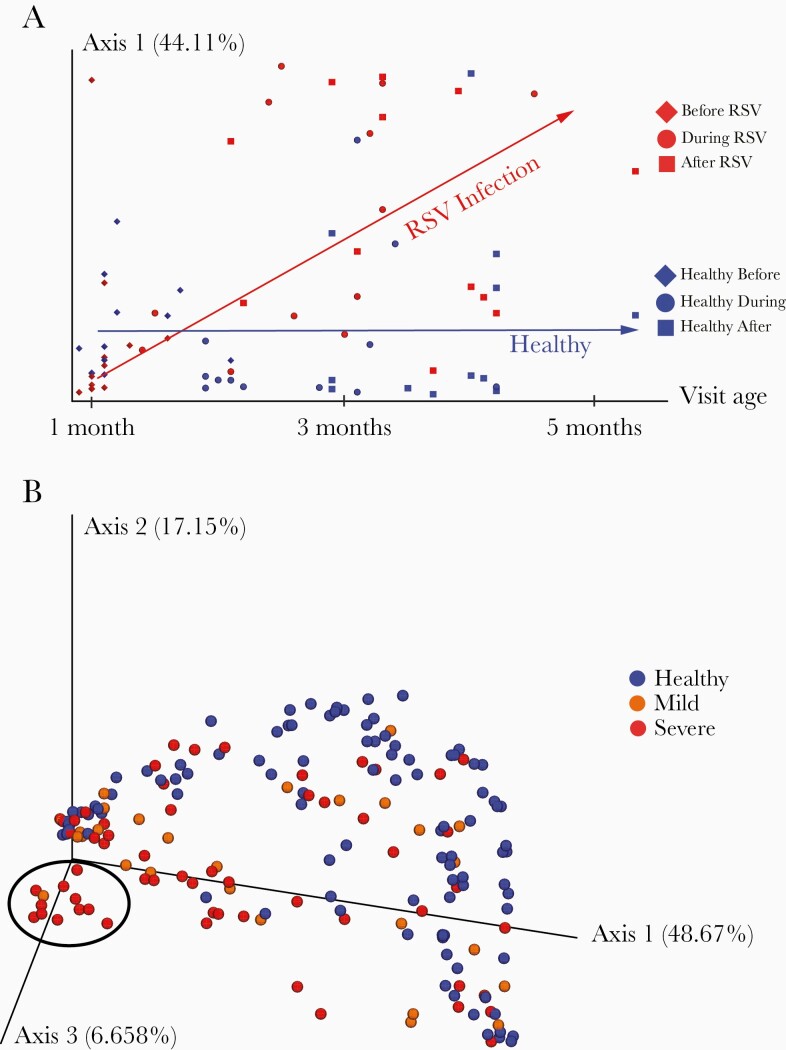
Methods: We carried out 16S rRNA microbiota profiling of infants in the first year of life from (1) a cross-sectional cohort of 89 RSV-infected infants sampled during illness and 102 matched healthy controls, and (2) a matched longitudinal cohort of 12 infants who developed RSV infection and 12 who did not, sampled before, during, and after infection.
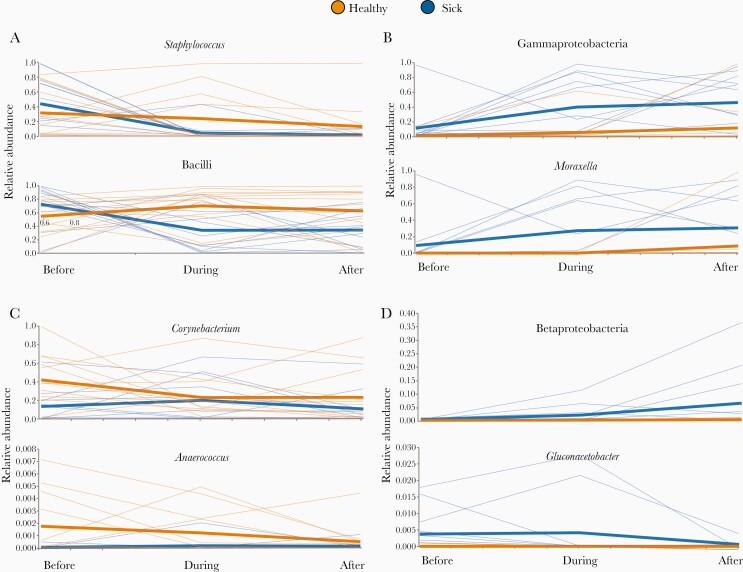
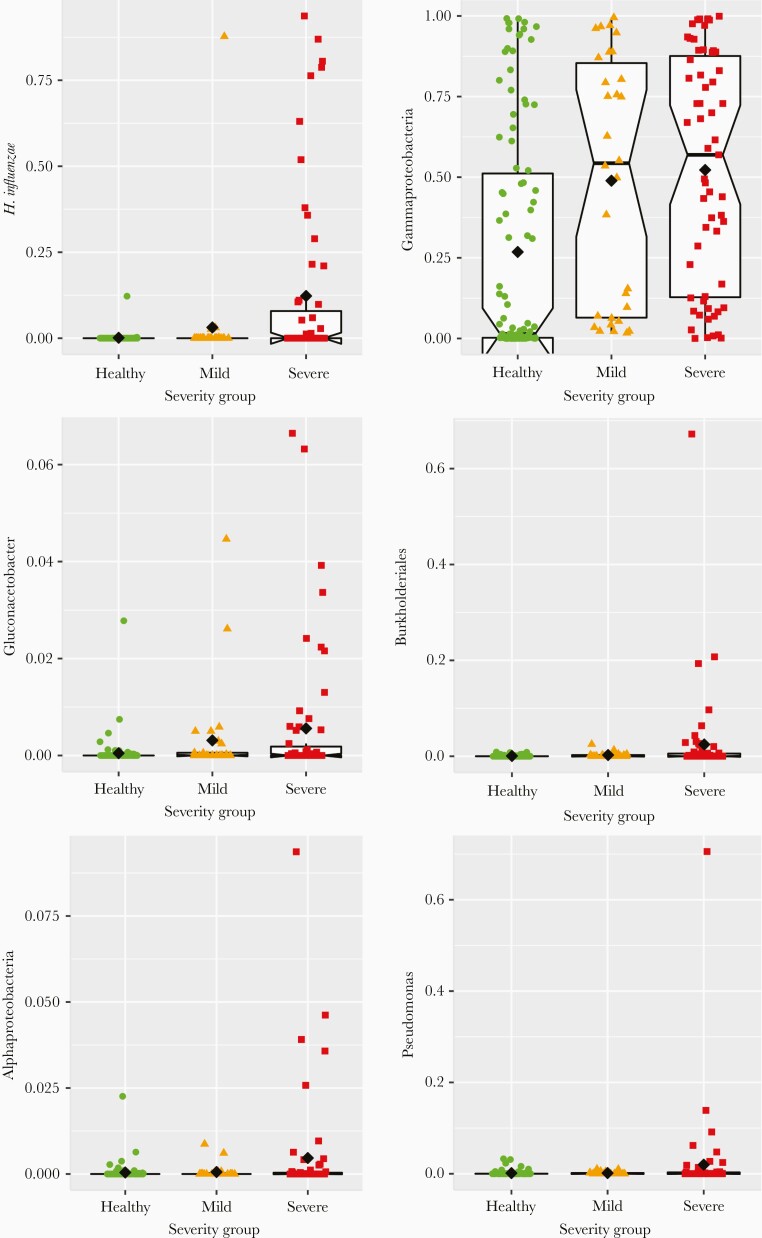
Results: We identified 12 taxa significantly associated with RSV infection. All 12 taxa were differentially abundant during infection, with 8 associated with disease severity. Nasal microbiota composition was more discriminative of healthy vs infected than of disease severity.
Conclusions: Our findings elucidate the chronology of nasal microbiota dysbiosis and suggest an altered developmental trajectory associated with RSV infection. Microbial temporal dynamics reveal indicators of disease risk, correlates of illness and severity, and impact of RSV infection on microbiota composition.
Keywords: microbiota; RSV; infant respiratory disease.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
