

Case report: multiple and atypical amoebic cerebral abscesses resistant to treatment
- PMID: 32928130
- PMCID: PMC7490879
- DOI: 10.1186/s12879-020-05391-y
Case report: multiple and atypical amoebic cerebral abscesses resistant to treatment
Abstract
Background: The parasite Entamoeba histolytica is the causal agent of amoebiasis, a worldwide emerging disease. Amebic brain abscess is a form of invasive amebiasis that is both rare and frequently lethal. This condition always begins with the infection of the colon by E. histolytica trophozoites, which subsequently travel through the bloodstream to extraintestinal tissues.
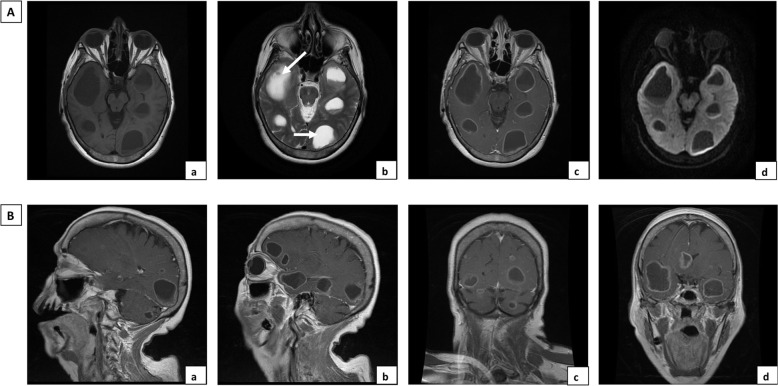
Case presentation: We report a case of a 71-year-old female who reported an altered state of consciousness, disorientation, sleepiness and memory loss. She had no history of hepatic or intestinal amoebiasis. A preliminary diagnosis of colloidal vesicular phase neurocysticercosis was made based on nuclear magnetic resonance imaging (NMRI). A postsurgery immunofluorescence study was positive for the 140 kDa fibronectin receptor of E. histolytica, although a serum analysis by ELISA was negative for IgG antibodies against this parasite. A specific E. histolytica 128 bp rRNA gene was identified by PCR in biopsy tissue. The final diagnosis was cerebral amoebiasis. The patient underwent neurosurgery to eliminate amoebic abscesses and was then given a regimen of metronidazole, ceftriaxone and dexamethasone for 4 weeks after the neurosurgery. However, a rapid decline in her condition led to death.
Conclusions: The present case of an individual with a rare form of cerebral amoebiasis highlights the importance of performing immunofluorescence, NMRI and PCR if a patient has brain abscess and a poorly defined diagnosis. Moreover, the administration of corticosteroids to such patients can often lead to a rapid decline in their condition.
Keywords: 140 kDa fibronectin receptor; Brain abscess; Cerebral amoebiasis; Entamoeba histolytica; NMRI; PCR.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures




Similar articles
-
Clinical case of cerebral amebiasis caused by E. histolytica.Parasitol Res. 2012 Mar;110(3):1291-6. doi: 10.1007/s00436-011-2617-8. Epub 2011 Aug 26. Parasitol Res. 2012. PMID: 21870245
-
Brain abscess due to infection with Entamoeba histolytica.Am J Trop Med Hyg. 1994 Aug;51(2):180-2. doi: 10.4269/ajtmh.1994.51.180. Am J Trop Med Hyg. 1994. PMID: 7915500
-
Detection of excretory Entamoeba histolytica DNA in the urine, and detection of E. histolytica DNA and lectin antigen in the liver abscess pus for the diagnosis of amoebic liver abscess.BMC Microbiol. 2007 May 18;7:41. doi: 10.1186/1471-2180-7-41. BMC Microbiol. 2007. PMID: 17511859 Free PMC article.
-
[Amebiasis].Ugeskr Laeger. 2000 Mar 13;162(11):1537-41. Ugeskr Laeger. 2000. PMID: 10868107 Review. Danish.
-
Thoracic amebiasis.Clin Chest Med. 2002 Jun;23(2):479-92. doi: 10.1016/s0272-5231(01)00008-9. Clin Chest Med. 2002. PMID: 12092041 Review.
Cited by
-
An Overview of Mucosa-Associated Protozoa: Challenges in Chemotherapy and Future Perspectives.Front Cell Infect Microbiol. 2022 Apr 25;12:860442. doi: 10.3389/fcimb.2022.860442. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 35548465 Free PMC article. Review.
-
Isolated amoebic brain abscess with excellent therapeutic response.Rev Soc Bras Med Trop. 2022 Apr 29;55:e00502022. doi: 10.1590/0037-8682-0050-2022. eCollection 2022. Rev Soc Bras Med Trop. 2022. PMID: 35522800 Free PMC article. No abstract available.
-
The Challenging Path to Diagnosing Extraintestinal Amoebiasis: A Case Report of an HIV-Infected Patient.Infect Drug Resist. 2023 Dec 8;16:7569-7574. doi: 10.2147/IDR.S442075. eCollection 2023. Infect Drug Resist. 2023. PMID: 38089958 Free PMC article.
-
An Unusual U2AF2 Inhibits Splicing and Attenuates the Virulence of the Human Protozoan Parasite Entamoeba histolytica.Front Cell Infect Microbiol. 2022 Jun 17;12:888428. doi: 10.3389/fcimb.2022.888428. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 35782149 Free PMC article.
-
Diversity and Plasticity of Virulent Characteristics of Entamoeba histolytica.Trop Med Infect Dis. 2023 Apr 29;8(5):255. doi: 10.3390/tropicalmed8050255. Trop Med Infect Dis. 2023. PMID: 37235303 Free PMC article. Review.
References
-
- WHO. Amoebiasis. Wkly Epidemiol Rec. 1997;72:97–98. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
