

Sentinel lymph node mapping using ICG fluorescence and cone beam CT - a feasibility study in a rabbit model of oral cancer
- PMID: 32928138
- PMCID: PMC7491106
- DOI: 10.1186/s12880-020-00507-x
Sentinel lymph node mapping using ICG fluorescence and cone beam CT - a feasibility study in a rabbit model of oral cancer
Abstract
Background: Current sentinel lymph node biopsy (SLNB) techniques, including use of radioisotopes, have disadvantages including the use of a radioactive tracer. Indocyanine green (ICG) based near-infrared (NIR) fluorescence imaging and cone beam CT (CBCT) have advantages for intraoperative use. However, limited literature exists regarding their use in head and neck cancer SLNB.
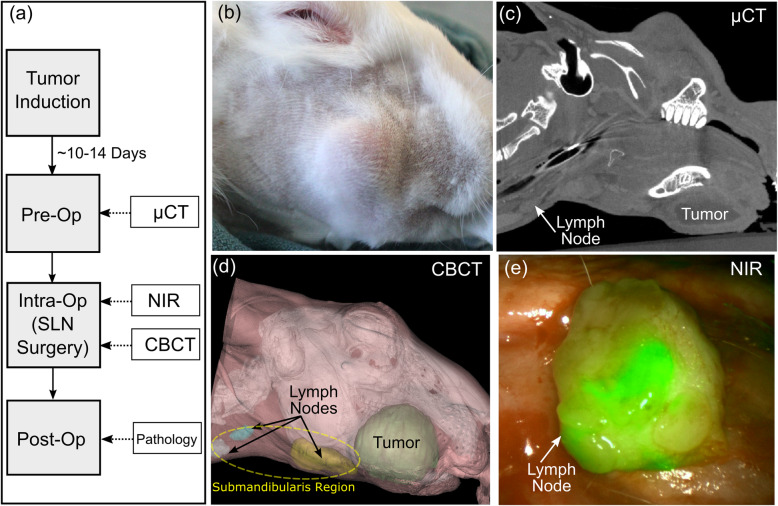
Methods: This was a prospective, non-randomized study using a rabbit oral cavity VX2 squamous cell carcinoma model (n = 10) which develops lymph node metastasis. Pre-operatively, images were acquired by MicroCT. During surgery, CBCT and NIR fluorescence imaging of ICG was used to map and guide the SLNB resection.
Results: Intraoperative use of ICG to guide fluorescence resection resulted in identification of all lymph nodes identified by pre-operative CT. CBCT was useful for near real time intraoperative imaging and 3D reconstruction.
Conclusions: This pre-clinical study further demonstrates the technical feasibility, limitations and advantages of intraoperative NIR-guided ICG imaging for SLN identification as a complementary method during head and neck surgery.
Keywords: Cone beam CT; Head and neck cancer; Head and neck surgery; Indocyanine green; Near-infrared fluorescence imaging; Sentinel lymph node biopsy.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


Similar articles
-
Robot-assisted real-time sentinel lymph node mapping in oral cavity cancer: preliminary experience.J Robot Surg. 2021 Jun;15(3):349-353. doi: 10.1007/s11701-020-01112-4. Epub 2020 Jun 27. J Robot Surg. 2021. PMID: 32594419
-
Utilization of Indocyanine Green to Aid in Identifying Sentinel Lymph Nodes in Merkel Cell Cancer.J Surg Res. 2018 Dec;232:365-368. doi: 10.1016/j.jss.2018.06.070. Epub 2018 Jul 18. J Surg Res. 2018. PMID: 30463742
-
[Diagnostic value of optical imaging combined with indocyanine green-guided sentinel lymph node biopsy in gastric cancer: a meta-analysis].Zhonghua Wei Chang Wai Ke Za Zhi. 2019 Dec 25;22(12):1196-1204. doi: 10.3760/cma.j.issn.1671-0274.2019.12.017. Zhonghua Wei Chang Wai Ke Za Zhi. 2019. PMID: 31874538 Chinese.
-
Diagnostic value of near-infrared or fluorescent indocyanine green guided sentinel lymph node mapping in gastric cancer: A systematic review and meta-analysis.J Surg Oncol. 2018 Dec;118(8):1243-1256. doi: 10.1002/jso.25285. Epub 2018 Oct 31. J Surg Oncol. 2018. PMID: 30380146
-
Diagnostic value of indocyanine green fluorescence guided sentinel lymph node biopsy in vulvar cancer: A systematic review.Gynecol Oncol. 2021 May;161(2):436-441. doi: 10.1016/j.ygyno.2021.01.031. Epub 2021 Feb 5. Gynecol Oncol. 2021. PMID: 33551201
Cited by
-
Cone Beam Computed Tomography in Oral Cancer: A Scoping Review.Diagnostics (Basel). 2025 May 29;15(11):1378. doi: 10.3390/diagnostics15111378. Diagnostics (Basel). 2025. PMID: 40506950 Free PMC article. Review.
-
Imaging Techniques in Pharmacological Precision Medicine.Handb Exp Pharmacol. 2023;280:213-235. doi: 10.1007/164_2023_641. Handb Exp Pharmacol. 2023. PMID: 36907970
-
Integrative lymph node-mimicking models created with biomaterials and computational tools to study the immune system.Mater Today Bio. 2022 Apr 21;14:100269. doi: 10.1016/j.mtbio.2022.100269. eCollection 2022 Mar. Mater Today Bio. 2022. PMID: 35514433 Free PMC article. Review.
-
DeepVinci: Organ and Tool Segmentation with Edge Supervision and a Densely Multi-Scale Pyramid Module for Robot-Assisted Surgery.Diagnostics (Basel). 2025 Jul 30;15(15):1917. doi: 10.3390/diagnostics15151917. Diagnostics (Basel). 2025. PMID: 40804883 Free PMC article.
-
Tumor Accumulation and Off-Target Biodistribution of an Indocyanine-Green Fluorescent Nanotracer: An Ex Vivo Study on an Orthotopic Murine Model of Breast Cancer.Int J Mol Sci. 2021 Feb 5;22(4):1601. doi: 10.3390/ijms22041601. Int J Mol Sci. 2021. PMID: 33562574 Free PMC article.
References
-
- Abu-Ghanem S, et al. Elective neck dissection vs observation in early-stage squamous cell carcinoma of the Oral tongue with no clinically apparent lymph node metastasis in the neck: a systematic review and meta-analysis. JAMA Otolaryngol Head Neck Surg. 2016;142(9):857–865. doi: 10.1001/jamaoto.2016.1281. - DOI - PubMed
-
- El Hage Chehade H, et al. Is sentinel lymph node biopsy a viable alternative to complete axillary dissection following neoadjuvant chemotherapy in women with node-positive breast cancer at diagnosis? An updated meta-analysis involving 3,398 patients. Am J Surg. 2016;212(5):969–981. doi: 10.1016/j.amjsurg.2016.07.018. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
