

Adaptive tutorials versus web-based resources in radiology: a mixed methods analysis in junior doctors of efficacy and engagement
- PMID: 32928196
- PMCID: PMC7491171
- DOI: 10.1186/s12909-020-02237-8
Adaptive tutorials versus web-based resources in radiology: a mixed methods analysis in junior doctors of efficacy and engagement
Abstract
Background: Radiology education is limited in undergraduate Medicine programs. Junior doctors might not have the necessary background to effectively order and interpret diagnostic imaging investigations. Furthermore, junior doctors are often time-poor, balancing clinical commitments with ongoing learning, leadership and teaching responsibilities. Previous studies have demonstrated the efficacy of radiology-themed online adaptive tutorials for senior medical students. Such adaptive tutorials might therefore be an efficient and effective form of radiology education for junior doctors.
Methods: A randomised controlled crossover trial was performed to evaluate the impact of adaptive tutorials on learning the indications for, and interpretation of, basic imaging studies, compared with peer-reviewed web-based resources. Ninety-one volunteer junior doctors, comprising 53 postgraduate year 1 (PGY 1) and 38 postgraduate year 2 (PGY 2), were randomly allocated into two groups. In the first phase of the trial, focusing on head CT, one group accessed adaptive tutorials while the other received web-based resources. In the second phase of the trial, focusing on chest CT, the groups crossed over. Following each phase of the trial, participants completed exam-style online assessments. At the conclusion of the study, participants also completed an online questionnaire regarding perceived engagement and efficacy of each type of educational resource.
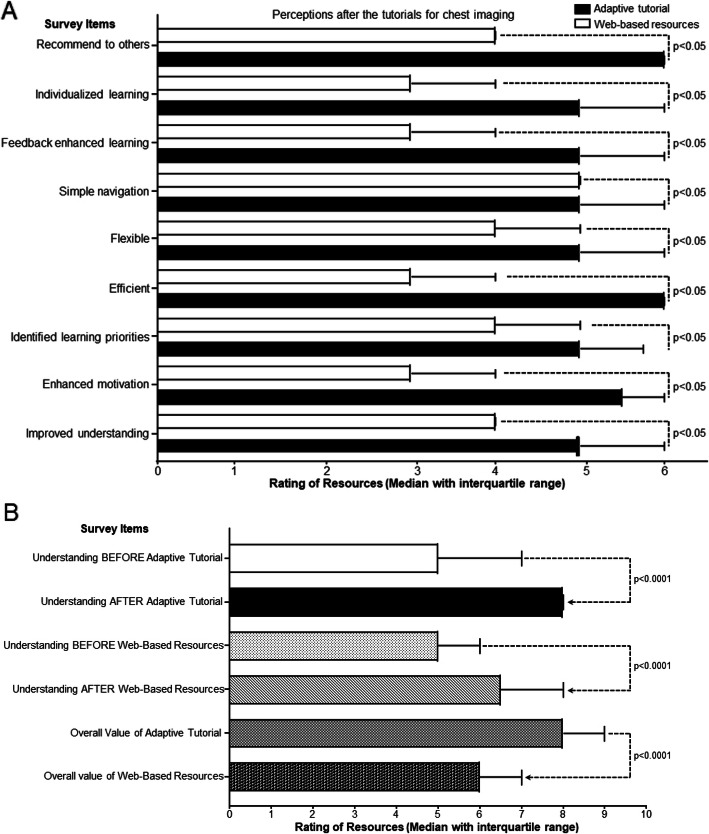
Results: Junior doctors completed the adaptive tutorials significantly faster than the relevant web-based resources for both head CT and chest CT (p = 0.03 and < 0.01 respectively). Mean quiz scores were higher in the groups receiving adaptive tutorials on head CT and chest CT (86.4% vs 83.5 and 77.7% vs 75% respectively). However, in contrast to previous studies in senior medical students, these differences were not statistically significant. Participants reported higher engagement and perceived value of adaptive tutorials, compared with web-based resources.
Conclusions: Adaptive tutorials are more time-efficient than existing web-based resources for learning radiology by junior doctors, while both types of resources were equally effective for learning in this cohort. Junior doctors found the adaptive tutorials more engaging and were more likely to recommend these resources to their colleagues.
Keywords: Adaptive tutorials; Diagnostic imaging; Junior doctors; Medical education; Radiology.
Conflict of interest statement
The authors declare they have no competing interests.
Figures



Similar articles
-
Adaptive Tutorials Versus Web-Based Resources in Radiology: A Mixed Methods Analysis of Efficacy and Engagement in Senior Medical Students.Acad Radiol. 2019 Oct;26(10):1421-1431. doi: 10.1016/j.acra.2019.02.021. Epub 2019 Apr 30. Acad Radiol. 2019. PMID: 31047791 Clinical Trial.
-
Adaptive Tutorials Versus Web-Based Resources in Radiology: A Mixed Methods Comparison of Efficacy and Student Engagement.Acad Radiol. 2015 Oct;22(10):1299-307. doi: 10.1016/j.acra.2015.07.002. Epub 2015 Aug 17. Acad Radiol. 2015. PMID: 26292916 Clinical Trial.
-
Cytopathology whole slide images and adaptive tutorials for senior medical students: a randomized crossover trial.Diagn Pathol. 2016 Jan 8;11:1. doi: 10.1186/s13000-016-0452-z. Diagn Pathol. 2016. PMID: 26746436 Free PMC article. Clinical Trial.
-
Web-based resources for critical care education.Crit Care Med. 2011 Mar;39(3):541-53. doi: 10.1097/CCM.0b013e318206b5b5. Crit Care Med. 2011. PMID: 21169819 Review.
-
Medical imaging education opportunities for junior doctors and non-radiologist clinicians: A review.J Med Imaging Radiat Oncol. 2021 Oct;65(6):710-718. doi: 10.1111/1754-9485.13266. Epub 2021 Jun 28. J Med Imaging Radiat Oncol. 2021. PMID: 34180148 Review.
Cited by
-
Comparative study of virtual and face-to-face training methods on the quality of healthcare services provided by Kermanshah pre-hospital emergency staff (EMS): randomized educational Intervention trial.BMC Med Educ. 2022 Mar 25;22(1):203. doi: 10.1186/s12909-022-03277-y. BMC Med Educ. 2022. PMID: 35337312 Free PMC article. Clinical Trial.
-
Improving the accuracy of emergency department clinicians in detecting SARS-COV-2 on chest X-rays using a bespoke virtual training platform.BMC Med Educ. 2025 Aug 6;25(1):1147. doi: 10.1186/s12909-025-07672-z. BMC Med Educ. 2025. PMID: 40770759 Free PMC article.
-
The effect of a training webinar on decreasing inter-observer variability in making a radiologic diagnosis of bronchiectasis.BMC Med Imaging. 2022 Aug 24;22(1):148. doi: 10.1186/s12880-022-00878-3. BMC Med Imaging. 2022. PMID: 36002806 Free PMC article.
-
What works in radiology education for medical students: a systematic review and meta-analysis.BMC Med Educ. 2024 Jan 10;24(1):51. doi: 10.1186/s12909-023-04981-z. BMC Med Educ. 2024. PMID: 38200489 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
