

The Capacity of the Ovarian Cancer Tumor Microenvironment to Integrate Inflammation Signaling Conveys a Shorter Disease-free Interval
- PMID: 32928797
- PMCID: PMC7923250
- DOI: 10.1158/1078-0432.CCR-20-1762
The Capacity of the Ovarian Cancer Tumor Microenvironment to Integrate Inflammation Signaling Conveys a Shorter Disease-free Interval
Abstract
Purpose: Ovarian cancer has one of the highest deaths to incidence ratios across all cancers. Initial chemotherapy is effective, but most patients develop chemoresistant disease. Mechanisms driving clinical chemo-response or -resistance are not well-understood. However, achieving optimal surgical cytoreduction improves survival, and cytoreduction is improved by neoadjuvant chemotherapy (NACT). NACT offers a window to profile pre- versus post-NACT tumors, which we used to identify chemotherapy-induced changes to the tumor microenvironment.
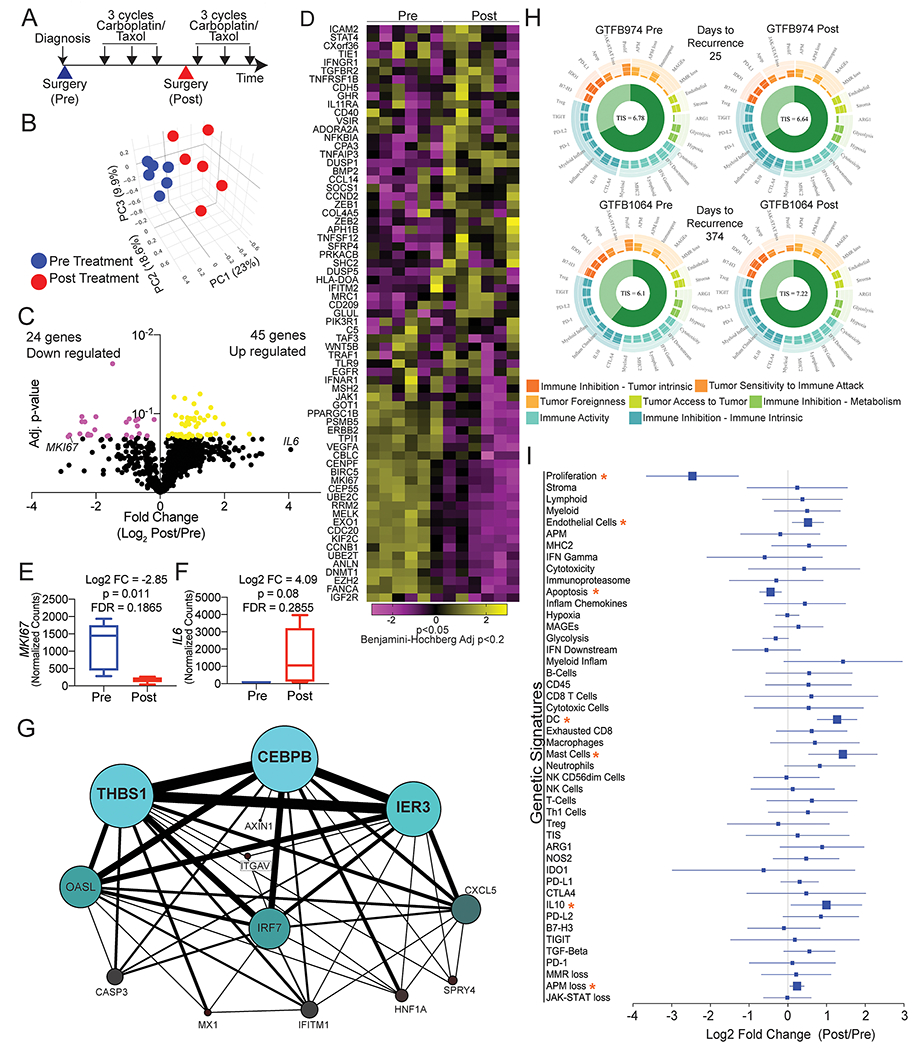
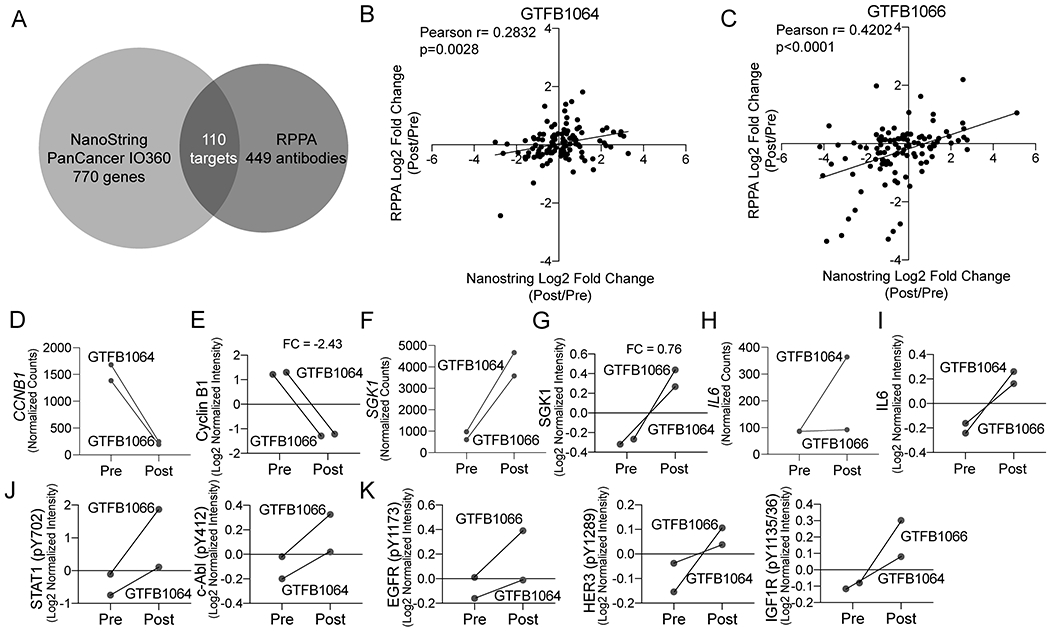
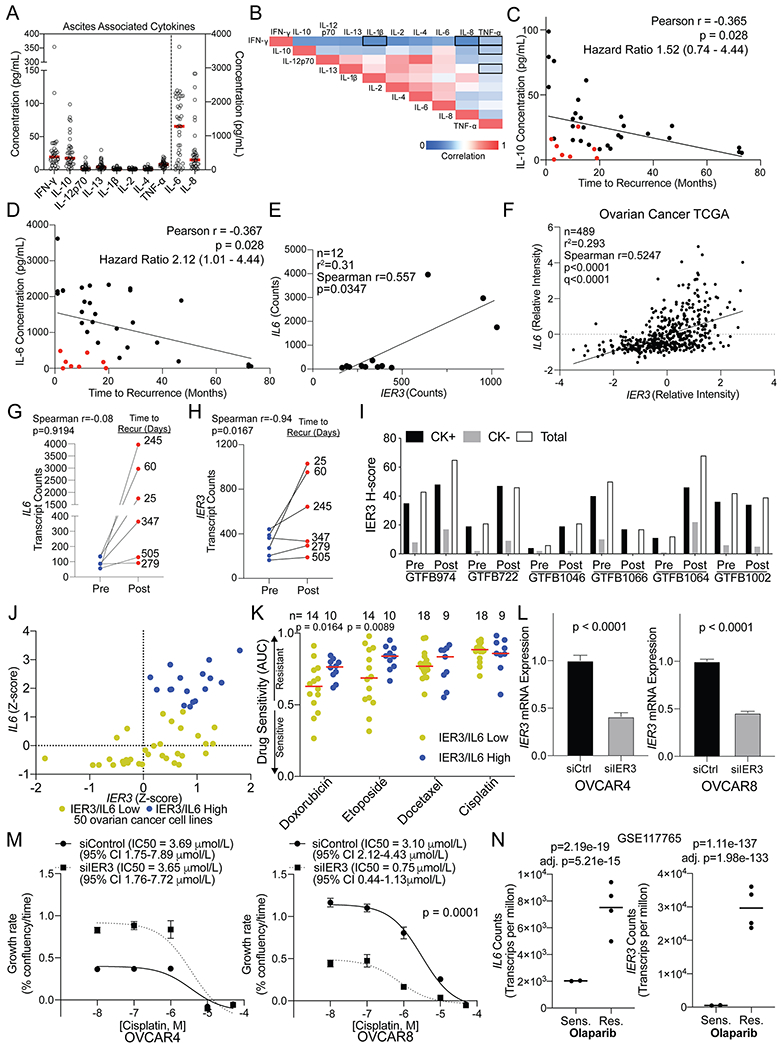
Experimental design: We obtained matched pre- and post-NACT archival tumor tissues from patients with high-grade serous ovarian cancer (patient, n = 6). We measured mRNA levels of 770 genes (756 genes/14 housekeeping genes, NanoString Technologies), and performed reverse phase protein array (RPPA) on a subset of matched tumors. We examined cytokine levels in pre-NACT ascites samples (n = 39) by ELISAs. A tissue microarray with 128 annotated ovarian tumors expanded the transcriptional, RPPA, and cytokine data by multispectral IHC.
Results: The most upregulated gene post-NACT was IL6 (16.79-fold). RPPA data were concordant with mRNA, consistent with elevated immune infiltration. Elevated IL6 in pre-NACT ascites specimens correlated with a shorter time to recurrence. Integrating NanoString (n = 12), RPPA (n = 4), and cytokine (n = 39) studies identified an activated inflammatory signaling network and induced IL6 and IER3 (immediate early response 3) post-NACT, associated with poor chemo-response and time to recurrence.
Conclusions: Multiomics profiling of ovarian tumor samples pre- and post-NACT provides unique insight into chemo-induced changes to the tumor microenvironment. We identified a novel IL6/IER3 signaling axis that may drive chemoresistance and disease recurrence.
©2020 American Association for Cancer Research.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures

References
-
- Siegel RL, Miller KD, and Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7–34. - PubMed
-
- Fagotti A, Ferrandina G, Fanfani F, Ercoli A, Lorusso D, Rossi M, et al. A laparoscopy-based score to predict surgical outcome in patients with advanced ovarian carcinoma: a pilot study. Ann Surg Oncol. 2006;13(8):1156–61. - PubMed
-
- Petrillo M, Vizzielli G, Fanfani F, Gallotta V, Cosentino F, Chiantera V, et al. Definition of a dynamic laparoscopic model for the prediction of incomplete cytoreduction in advanced epithelial ovarian cancer: proof of a concept. Gynecol Oncol. 2015;139(1):5–9. - PubMed
-
- Bian C, Yao K, Li L, Yi T, and Zhao X. Primary debulking surgery vs. neoadjuvant chemotherapy followed by interval debulking surgery for patients with advanced ovarian cancer. Arch Gynecol Obstet. 2016;293(1):163–8. - PubMed
-
- May T, Comeau R, Sun P, Kotsopoulos J, Narod SA, Rosen B, et al. A Comparison of Survival Outcomes in Advanced Serous Ovarian Cancer Patients Treated With Primary Debulking Surgery Versus Neoadjuvant Chemotherapy. Int J Gynecol Cancer. 2017;27(4):668–74. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
