

Neoadjuvant nivolumab plus ipilimumab in resectable non-small cell lung cancer
- PMID: 32929052
- PMCID: PMC7488786
- DOI: 10.1136/jitc-2020-001282
Neoadjuvant nivolumab plus ipilimumab in resectable non-small cell lung cancer
Abstract
Background: We conducted the first trial of neoadjuvant PD-1 blockade in resectable non-small cell lung cancer (NSCLC), finding nivolumab monotherapy to be safe and feasible with an encouraging rate of pathologic response. Building on these results, and promising data for nivolumab plus ipilimumab (anti-CTLA-4) in advanced NSCLC, we expanded our study to include an arm investigating neoadjuvant nivolumab plus ipilimumab.
Methods: Patients with resectable stage IB (≥4 cm)-IIIA (American Joint Committee on Cancer Tumor Node Metastases seventh edition), histologically confirmed, treatment-naïve NSCLC received nivolumab 3 mg/kg intravenously plus ipilimumab 1 mg/kg intravenously 6 weeks prior to planned resection. Nivolumab 3 mg/kg was given again approximately 4 and 2 weeks preoperatively. Primary endpoints were safety and feasibility with a planned enrollment of 15 patients. Pathologic response was a key secondary endpoint.
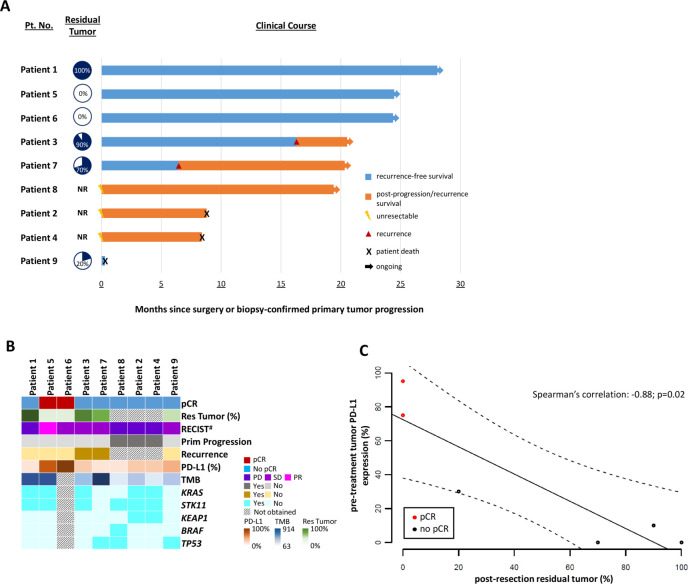
Results: While the treatment regimen was feasible per protocol, due to toxicity, the study arm was terminated early by investigator consensus after 9 of 15 patients were enrolled. All patients received every scheduled dose of therapy and were fit for planned surgery; however, 6 of 9 (67%) experienced treatment-related adverse events (TRAEs) and 3 (33%) experienced grade ≥3 TRAEs. Three of 9 patients (33%) had biopsy-confirmed tumor progression precluding definitive surgery. Of the 6 patients who underwent resection, 3 are alive and disease-free, 2 experienced recurrence and are actively receiving systemic treatment, and one died postoperatively due to acute respiratory distress syndrome. Two patients who underwent resection had tumor pathologic complete responses (pCRs) and continue to remain disease-free over 24 months since surgery. Pathologic response correlated with pre-treatment tumor PD-L1 expression, but not tumor mutation burden. Tumor KRAS/STK11 co-mutations were identified in 5 of 9 patients (59%), of whom two with disease progression precluding surgery had tumor KRAS/STK11/KEAP1 co-mutations.
Conclusions: Though treatment was feasible, due to toxicity the study arm was terminated early by investigator consensus. In light of this, and while the long-term disease-free status of patients who achieved pCR is encouraging, further investigation of neoadjuvant nivolumab plus ipilimumab in patients with resectable NSCLC requires the identification of predictive biomarkers that enrich for response.
Keywords: clinical trials as topic; immunotherapy; lung neoplasms; tumor biomarkers; tumor microenvironment.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JER has received grants from Conquer Cancer: The ASCO Foundation. VA has received grants from the National Institutes of Health, The LUNGevity Foundation, The V Foundation, Swim Across America, The Allegheny Health Network – Johns Hopkins Research Fund and the Maryland Department of Health and Mental Hygiene Cigarette Restitution Fund Program, Bristol-Myers Squibb, and Personal Genomic Diagnostics. KS has received personal fees from Illumina. JRW is the founder and owner of Resphera Biosciences LLC. SB has received personal fees from Bristol-Myers Squibb. DJ has been on the advisory boards of Diffusion Pharmaceuticals, Merck, and AstraZeneca. TM has received grants from Bristol-Myers Squibb, Surface Oncology, Kyn Therapeutics, Infinity Pharmaceuticals, Peregrine Pharmaceuticals, Adaptive BioTechnologies, Leap Therapeutics, and Aprea; has received personal fees from Leap Therapeutics, Immunos Therapeutics, and Pfizer; is co-founder and holds equity in Imvaq Therapeutics; and has filed patents for work related to PD-1 and CTLA-4. JT has received grants from Akoya Biosciences and Bristol-Myers Squibb, has received non-financial support from Akoya Biosciences, and has been on the advisory boards of Bristol-Myers Squibb, Merck, AstraZeneca, Compugen, and Regeneron. VEV has received grants from the National Institutes of Health, The Commonwealth Foundation, and Bloomberg–Kimmel Institute for Cancer Immunotherapy; has been on the advisory boards of Bristol-Myers Squibb, Genentech, Merck, and Takeda Pharmaceuticals; and is the founder, serves on board of directors and owns stock in Delfi Diagnostics and Personal Genome Diagnostics. GR has received personal fees from Medicago and owns stock in Johnson & Johnson. PI has received grants from Bristol-Myers Squibb and Biomarker Strategies, LLC; has received personal fees from AbbVie, AstraZeneca, Bayer, Veran Medical Technologies Inc., and Roche Diagnostics; and has been on the advisory boards of AstraZeneca and Guardant Health. DMP and ST have received research grants from Bristol-Myers Squibb and Compugen; have received personal fees from Aduro Biotech, Five Prime Therapeutics, Tizona Therapeutics, DNAtrix, RAPT, WindMIL, Dragonfly Therapeutics, Ervaxx, Amgen, MedImmune, Merck, Compugen, Dynavax, Immunomic Therapeutics, Janssen Oncology, Immunocore, Bristol-Myers Squibb, Arbor Pharmaceuticals, and NexImmune; and own equity in Aduro Biotech, Potenza Therapeutics, Five Prime Therapeutics, Tizona Therapeutics, DNAtrix, RAPT, WindMIL, Dragonfly Therapeutics, Ervaxx, and Trieza Therapeutics. JN has received grants from AstraZeneca and Merck; has been on the advisory boards of AstraZeneca, Bristol Myers-Squibb, and Genentech/Roche; and has received personal fees from AstraZeneca, Bristol-Myers Squibb, and Merck. BL has received grants from Eli Lilly, Genentech, Bristol-Myers Squibb, AstraZeneca, Turning Point Therapeutics, and Amgen; and has received personal fees from Eli Lilly, Genentech, AstraZeneca, Celgene, Pfizer, Merck, Novartis, and Takeda. MH has received grants from Bristol-Myers Squibb; has received personal fees from Bristol-Myers Squibb, Merck, AstraZeneca, Genentech/Roche, Nektar, Syndax, Mirati, Shattuck Labs, Immunai, Blueprint Medicines, Achilles, Arcus, and Eli Lilly; owns equity in Shattuck Labs, Immunai, and Arcus; and has filed patents related to the use of tumor mutation burden to predict response to immunotherapy. JRB has received grants from AstraZeneca, Bristol-Myers Squibb, Genentech/Roche, Merck, RAPT Therapeutics, Inc., and Revolution Medicines; has received personal fees from Genentech/Roche; has been on the advisory boards of Amgen, Bristol-Myers Squibb, Genentech/Roche, Eli Lilly, GlaxoSmithKline, Merck, and Sanofi; and has been on the Data and Safety Monitory boards of GlaxoSmithKline and Sanofi. JEC has received grants from the National Institutes of Health; and has also received grants and personal fees from Merck, Bristol-Myers Squibb, Genentech, and AstraZeneca. PMF has received grants from the LUNGevity Foundation, Stand Up To Cancer, AstraZeneca, Bristol-Myers Squibb, Kyowa, Novartis, and Corvus; and has been on the advisory boards of Abbvie, AstraZeneca, and Bristol-Myers Squibb. The remaining authors declare no conflicts of interest.
Figures
References
-
- Remon J, Passiglia F, Ahn MJ, et al. . Immune checkpoint inhibitors in thoracic malignancies: review of the existing evidence by an IASLC expert panel and recommendations. J Thorac Oncol 2020. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous