

Validation of reference genes for expression analysis in a murine trauma model combining traumatic brain injury and femoral fracture
- PMID: 32929099
- PMCID: PMC7490670
- DOI: 10.1038/s41598-020-71895-x
Validation of reference genes for expression analysis in a murine trauma model combining traumatic brain injury and femoral fracture
Abstract
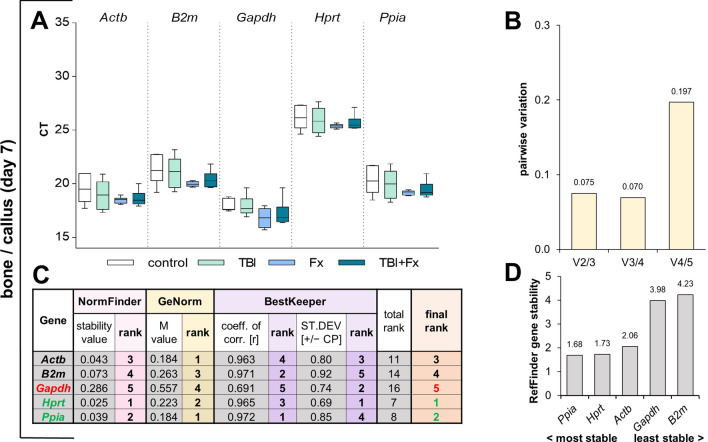
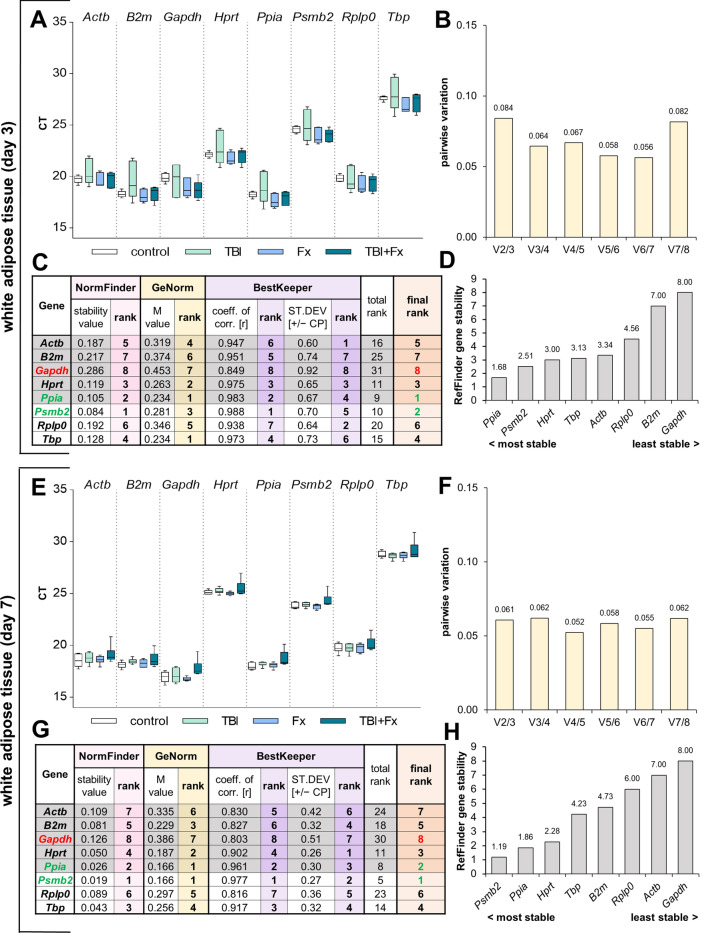
Systemic and local posttraumatic responses are often monitored on mRNA expression level using quantitative real-time PCR (qRT-PCR), which requires normalisation to adjust for confounding sources of variability. Normalisation requests reference (housekeeping) genes stable throughout time and divergent experimental conditions in the tissue of interest, which are crucial for a reliable and reproducible gene expression analysis. Although previous animal studies analysed reference genes following isolated trauma, this multiple-trauma gene expression analysis provides a notable study analysing reference genes in primarily affected (i.e. bone/fracture callus and hypothalamus) and secondarily affected organs (i.e. white adipose tissue, liver, muscle and spleen), following experimental long bone fracture and traumatic brain injury. We considered tissue-specific and commonly used top-ranked reference candidates from different functional groups that were evaluated applying the established expression stability analysis tools NormFinder, GeNorm, BestKeeper and RefFinder. In conclusion, reference gene expression in primary organs is highly time point as well as tissue-specific, and therefore requires careful evaluation for qRT-PCR analysis. Furthermore, the general application of Ppia, particularly in combination with a second reference gene, is strongly recommended for the analysis of systemic effects in the case of indirect trauma affecting secondary organs through local and systemic pathophysiological responses.
Conflict of interest statement
The authors declare no competing interests.
Figures





References
-
- 4World-Health-Organization. Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region 2000–2016 (2018).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
