

Management of Graves Thyroidal and Extrathyroidal Disease: An Update
- PMID: 32929476
- PMCID: PMC7543578
- DOI: 10.1210/clinem/dgaa646
Management of Graves Thyroidal and Extrathyroidal Disease: An Update
Abstract
Context: Invited update on the management of systemic autoimmune Graves disease (GD) and associated Graves orbitopathy (GO).
Evidence acquisition: Guidelines, pertinent original articles, systemic reviews, and meta-analyses.
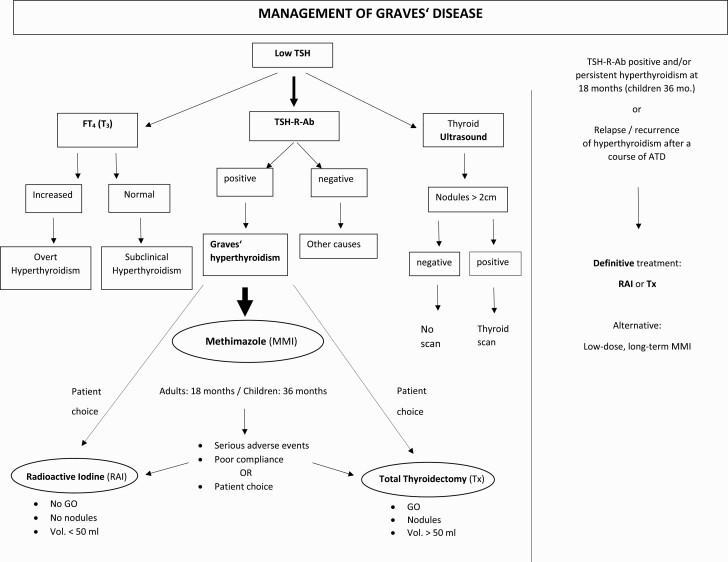
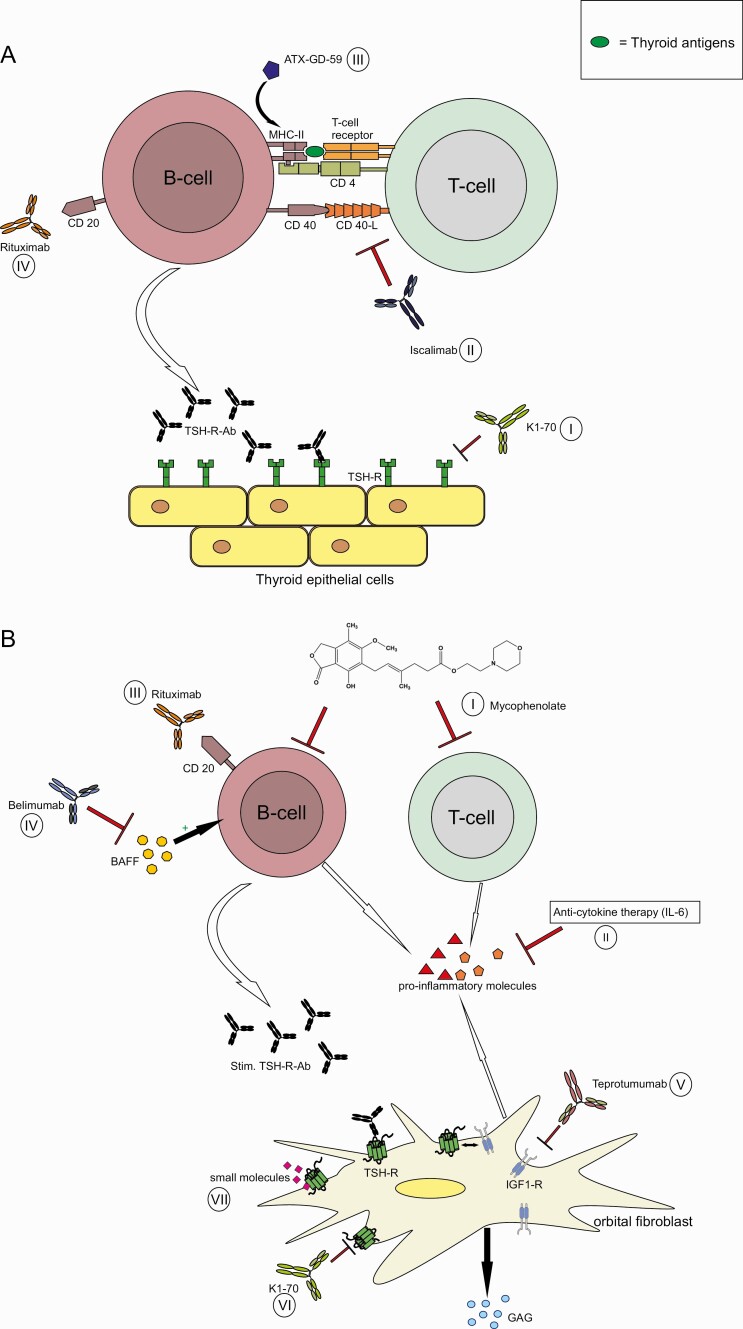
Evidence synthesis: Thyrotropin receptor antibodies (TSH-R-Abs), foremost the stimulatory TSH-R-Abs, are a specific biomarker for GD. Their measurement assists in the differential diagnosis of hyperthyroidism and offers accurate and rapid diagnosis of GD. Thyroid ultrasound is a sensitive imaging tool for GD. Worldwide, thionamides are the favored treatment (12-18 months) of newly diagnosed GD, with methimazole (MMI) as the preferred drug. Patients with persistently high TSH-R-Abs and/or persistent hyperthyroidism at 18 months, or with a relapse after completing a course of MMI, can opt for a definitive therapy with radioactive iodine (RAI) or total thyroidectomy (TX). Continued long-term, low-dose MMI administration is a valuable and safe alternative. Patient choice, both at initial presentation of GD and at recurrence, should be emphasized. Propylthiouracil is preferred to MMI during the first trimester of pregnancy. TX is best performed by a high-volume thyroid surgeon. RAI should be avoided in GD patients with active GO, especially in smokers. Recently, a promising therapy with an anti-insulin-like growth factor-1 monoclonal antibody for patients with active/severe GO was approved by the Food and Drug Administration. COVID-19 infection is a risk factor for poorly controlled hyperthyroidism, which contributes to the infection-related mortality risk. If GO is not severe, systemic steroid treatment should be postponed during COVID-19 while local treatment and preventive measures are offered.
Conclusions: A clear trend towards serological diagnosis and medical treatment of GD has emerged.
Keywords: Graves disease; TSH receptor antibodies; antithyroid drugs; diagnosis; management; radioactive iodine; thyroidectomy; treatment.
© The Author(s) 2020. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- Bahn Chair RS, Burch HB, Cooper DS, et al. ; American Thyroid Association; American Association of Clinical Endocrinologists . Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Thyroid. 2011;21(6):593-646. - PubMed
-
- Bartalena L. Diagnosis and management of Graves disease: a global overview. Nat Rev Endocrinol. 2013;9(12):724-734. - PubMed
-
- Nyström HF, Jansson S, Berg G. Incidence rate and clinical features of hyperthyroidism in a long-term iodine sufficient area of Sweden (Gothenburg) 2003-2005. Clin Endocrinol (Oxf). 2013;78(5):768-776. - PubMed
-
- McLeod DS, Caturegli P, Cooper DS, Matos PG, Hutfless S. Variation in rates of autoimmune thyroid disease by race/ethnicity in US military personnel. JAMA. 2014;311(15):1563-1565. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
