

Flotetuzumab as salvage immunotherapy for refractory acute myeloid leukemia
- PMID: 32929488
- PMCID: PMC7885824
- DOI: 10.1182/blood.2020007732
Flotetuzumab as salvage immunotherapy for refractory acute myeloid leukemia
Abstract
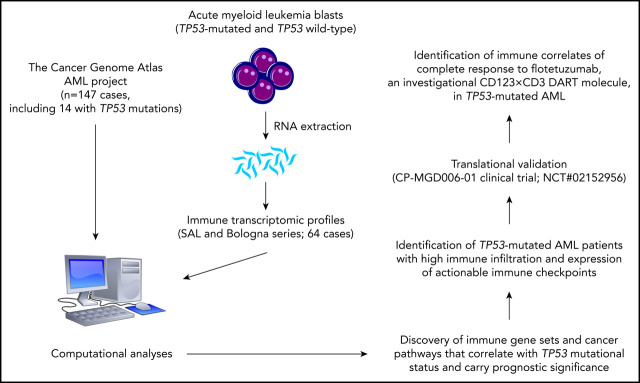
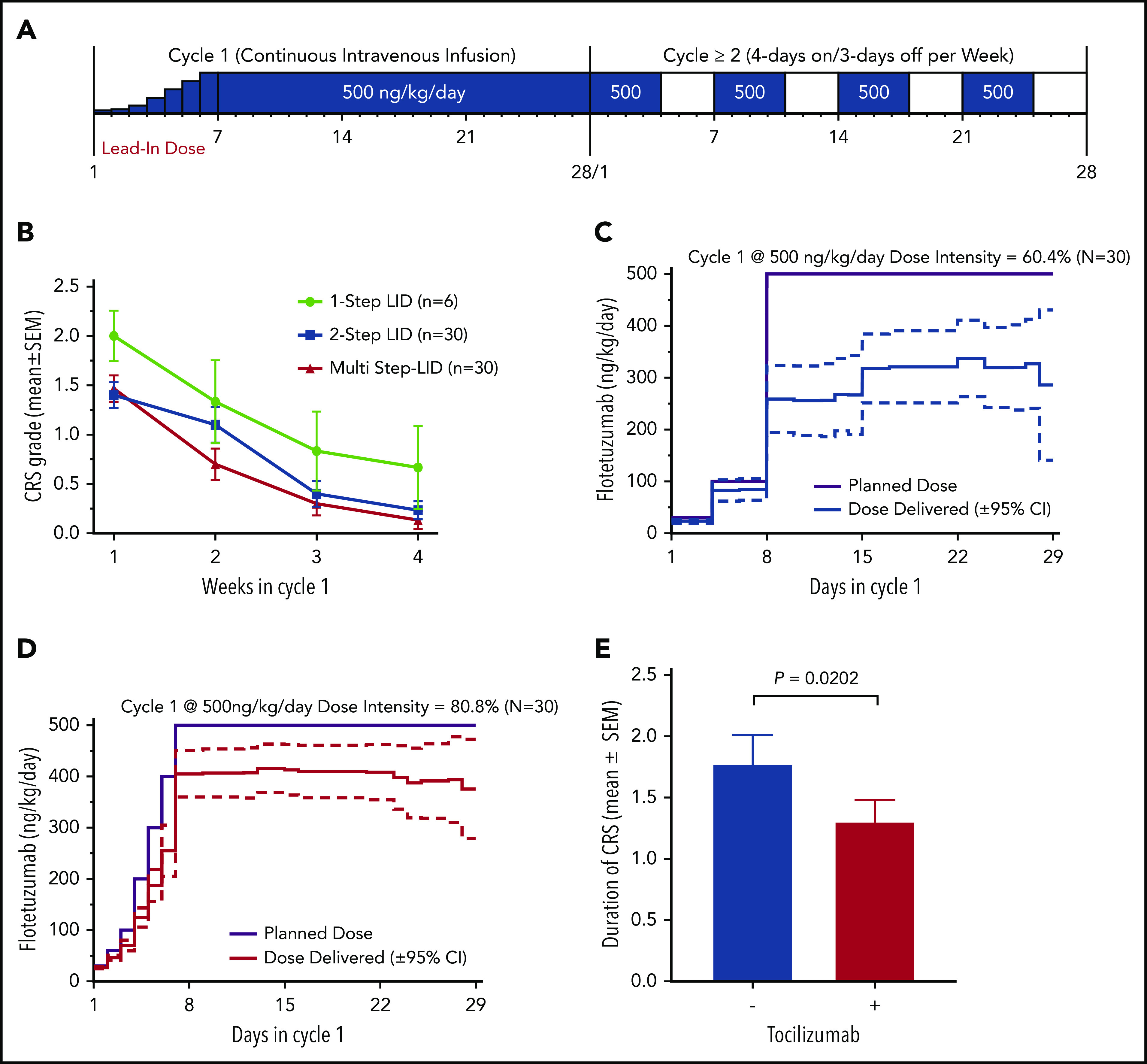
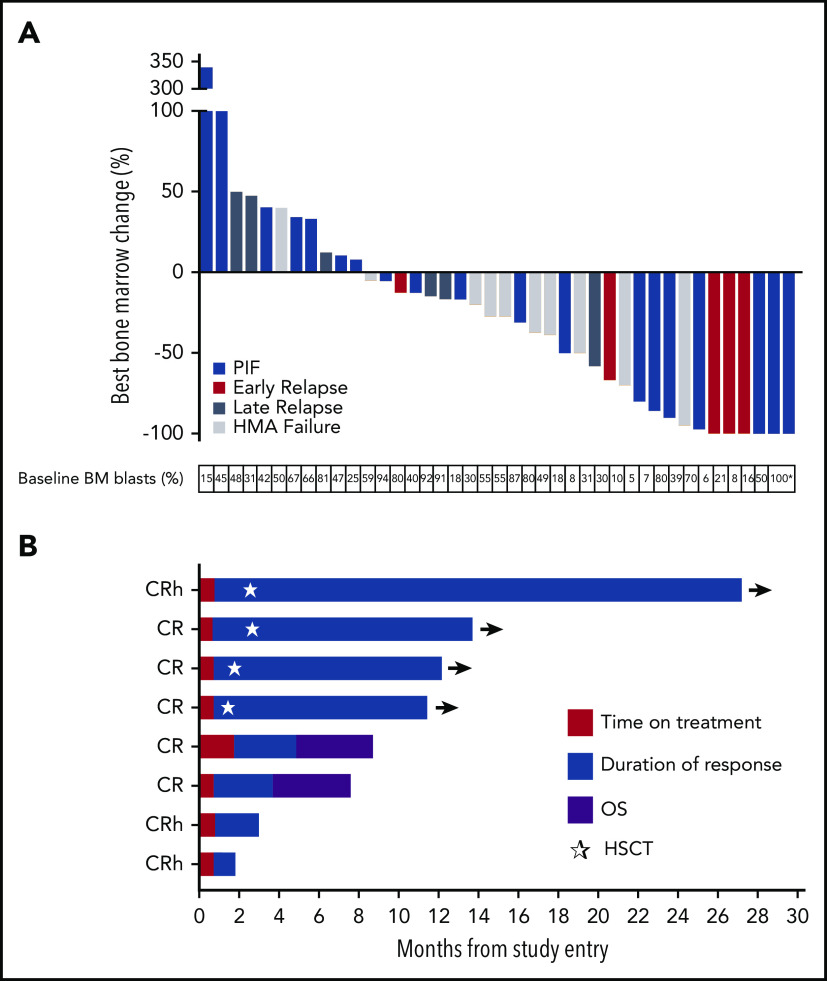
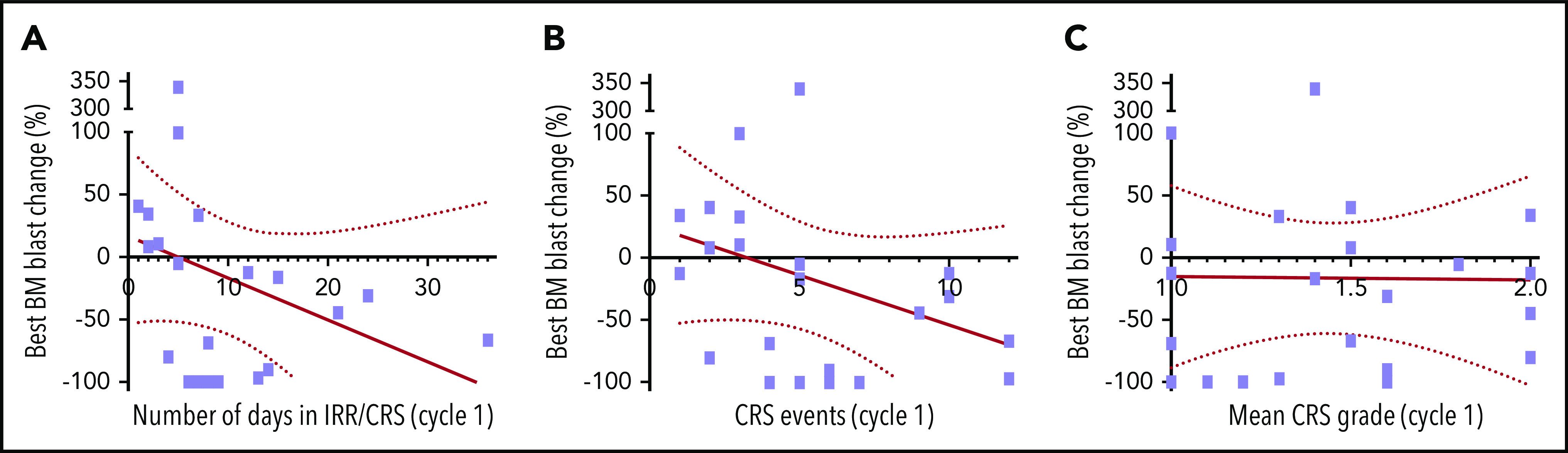
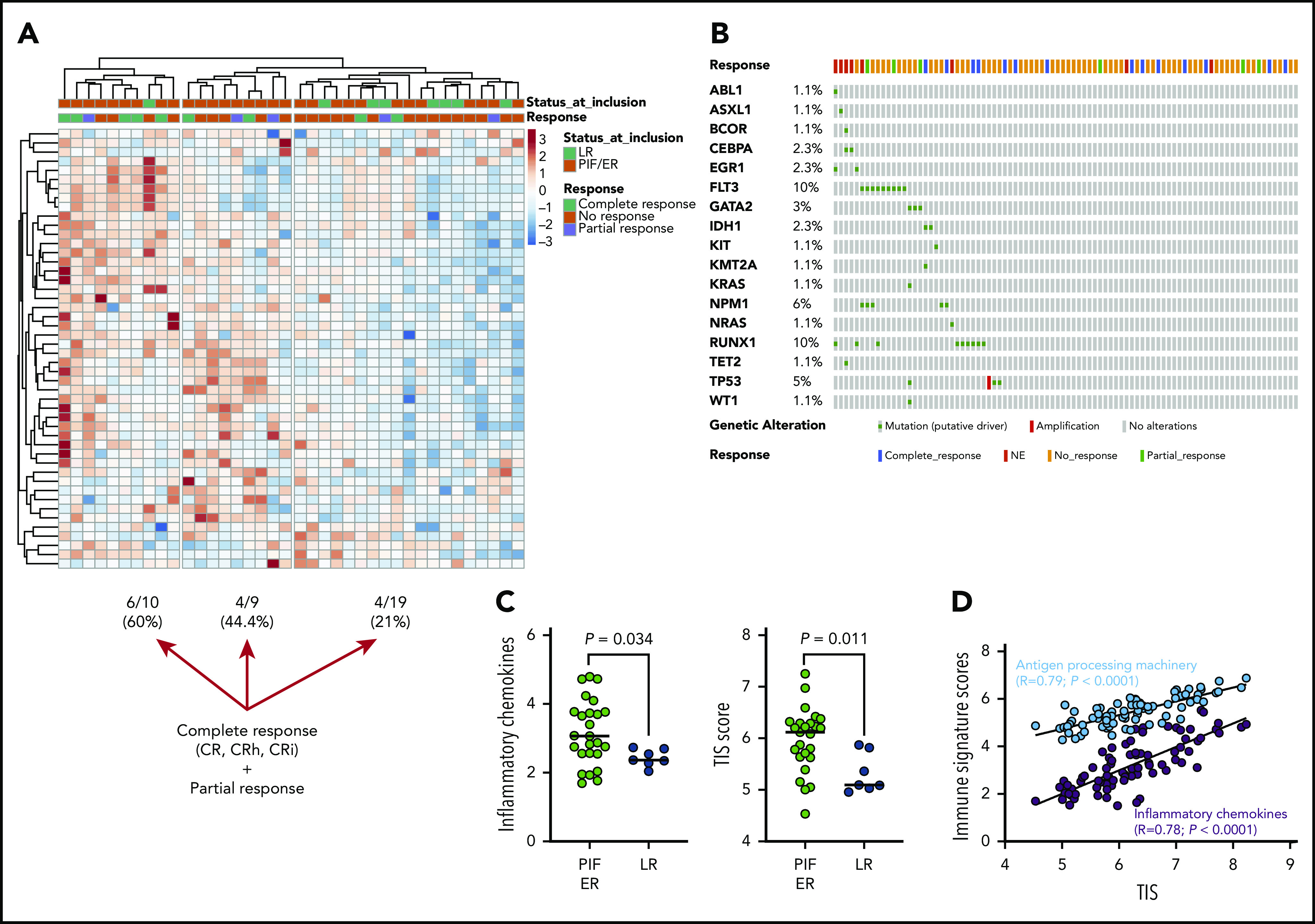
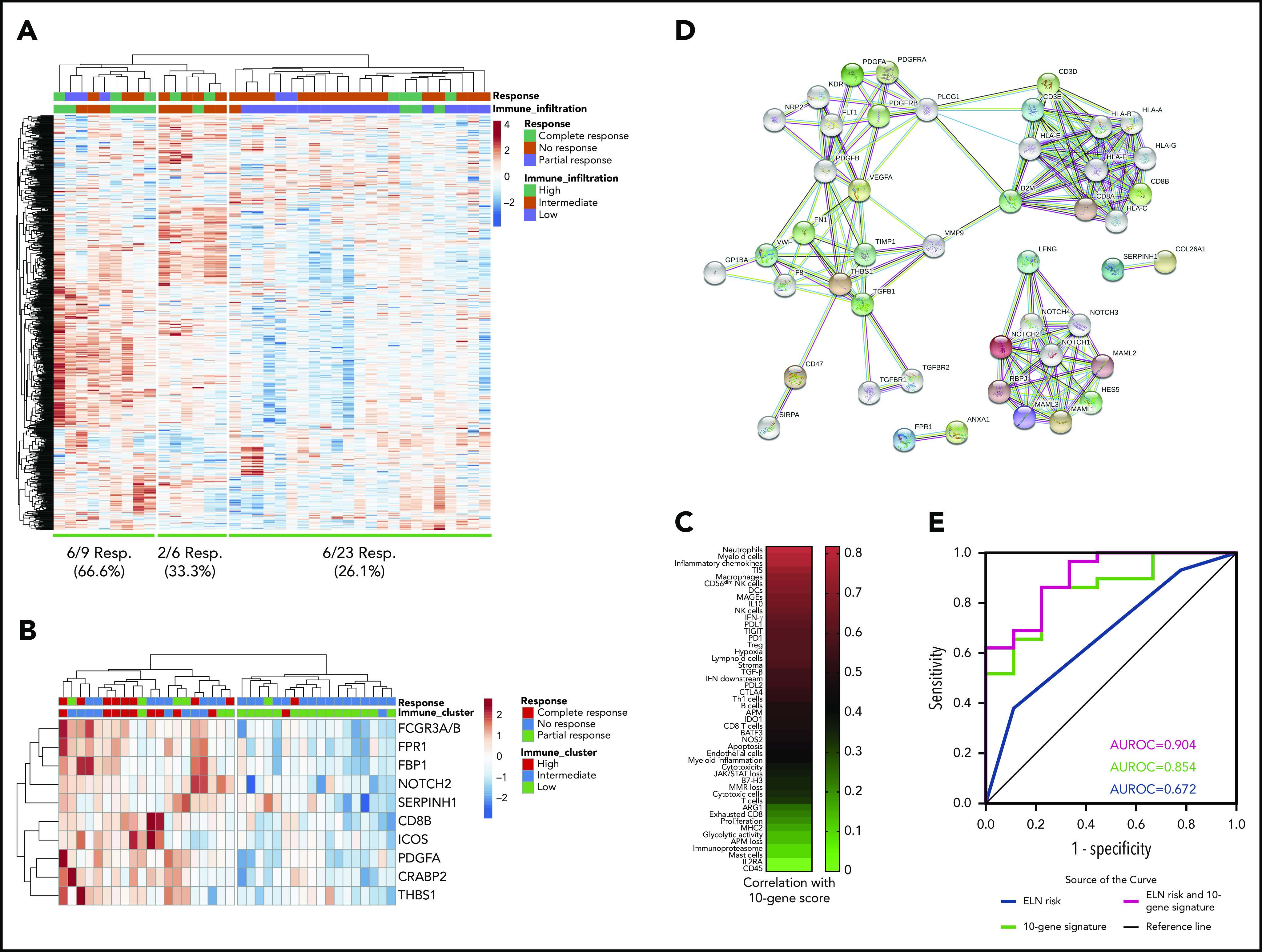
Approximately 50% of acute myeloid leukemia (AML) patients do not respond to induction therapy (primary induction failure [PIF]) or relapse after <6 months (early relapse [ER]). We have recently shown an association between an immune-infiltrated tumor microenvironment (TME) and resistance to cytarabine-based chemotherapy but responsiveness to flotetuzumab, a bispecific DART antibody-based molecule to CD3ε and CD123. This paper reports the results of a multicenter, open-label, phase 1/2 study of flotetuzumab in 88 adults with relapsed/refractory AML: 42 in a dose-finding segment and 46 at the recommended phase 2 dose (RP2D) of 500 ng/kg per day. The most frequent adverse events were infusion-related reactions (IRRs)/cytokine release syndrome (CRS), largely grade 1-2. Stepwise dosing during week 1, pretreatment dexamethasone, prompt use of tocilizumab, and temporary dose reductions/interruptions successfully prevented severe IRR/CRS. Clinical benefit accrued to PIF/ER patients showing an immune-infiltrated TME. Among 30 PIF/ER patients treated at the RP2D, the complete remission (CR)/CR with partial hematological recovery (CRh) rate was 26.7%, with an overall response rate (CR/CRh/CR with incomplete hematological recovery) of 30.0%. In PIF/ER patients who achieved CR/CRh, median overall survival was 10.2 months (range, 1.87-27.27), with 6- and 12-month survival rates of 75% (95% confidence interval [CI], 0.450-1.05) and 50% (95% CI, 0.154-0.846). Bone marrow transcriptomic analysis showed that a parsimonious 10-gene signature predicted CRs to flotetuzumab (area under the receiver operating characteristic curve = 0.904 vs 0.672 for the European LeukemiaNet classifier). Flotetuzumab represents an innovative experimental approach associated with acceptable safety and encouraging evidence of activity in PIF/ER patients. This trial was registered at www.clinicaltrials.gov as #NCT02152956.
© 2021 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: J.M., T.C., E.F., K.G., J.Z., O.B., K.J., K.T., P.K., M.K., E.B., and J.K.D.-M. are employees of MacroGenics Inc (Rockville, MD). S.E.C. is an employee of NanoString Technologies Inc (Seattle, WA). The remaining authors declare no competing financial interests.
Figures
Comment in
-
DARTs point the way forward in AML.Blood. 2021 Feb 11;137(6):720-721. doi: 10.1182/blood.2020009020. Blood. 2021. PMID: 33570611 No abstract available.
References
-
- Döhner H, Weisdorf DJ, Bloomfield CD. Acute myeloid leukemia. N Engl J Med. 2015;373(12):1136-1152. - PubMed
-
- Jabbour E, Garcia-Manero G, Cortes J, et al. Twice-daily fludarabine and cytarabine combination with or without gentuzumab ozogamicin is effective in patients with relapsed/refractory acute myeloid leukemia, high-risk myelodysplastic syndrome, and blast- phase chronic myeloid leukemia. Clin Lymphoma Myeloma Leuk. 2012;12(4):244-251. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
