

Aspects of colorectal cancer screening, methods, age and gender
- PMID: 32929813
- PMCID: PMC8048936
- DOI: 10.1111/joim.13171
Aspects of colorectal cancer screening, methods, age and gender
Abstract
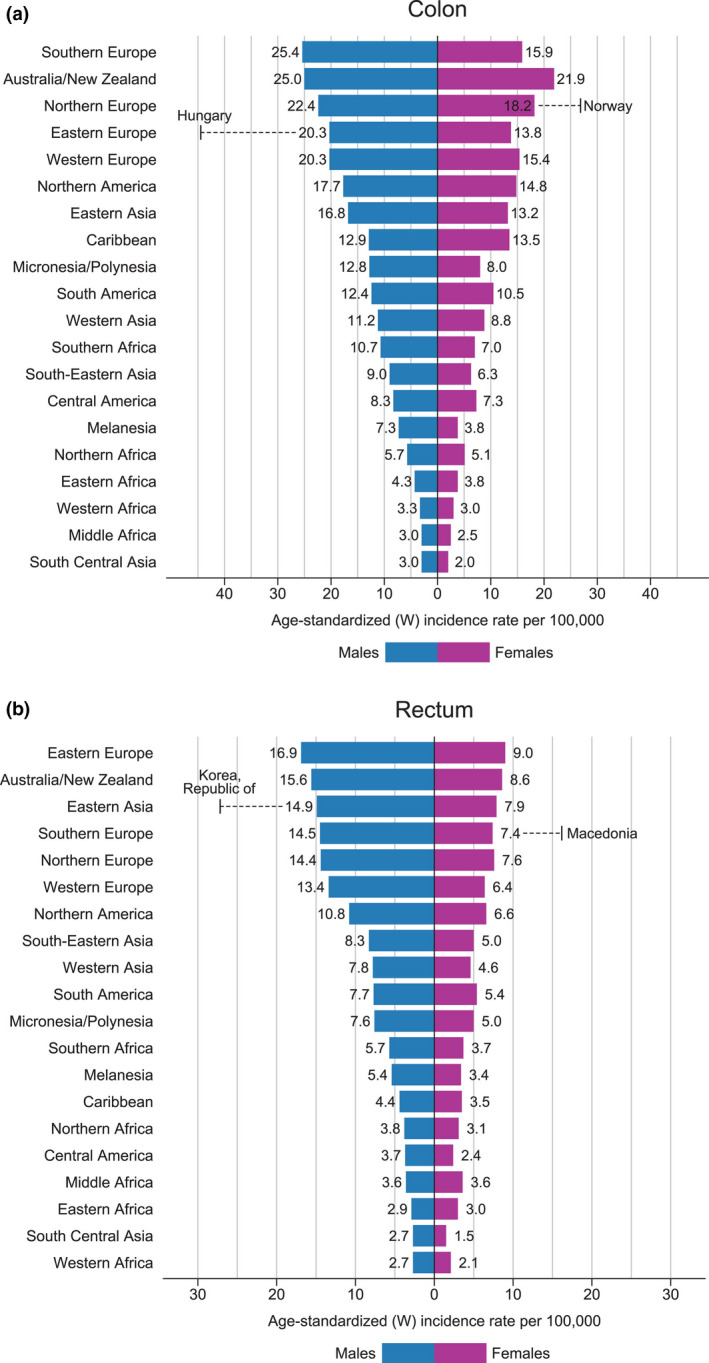
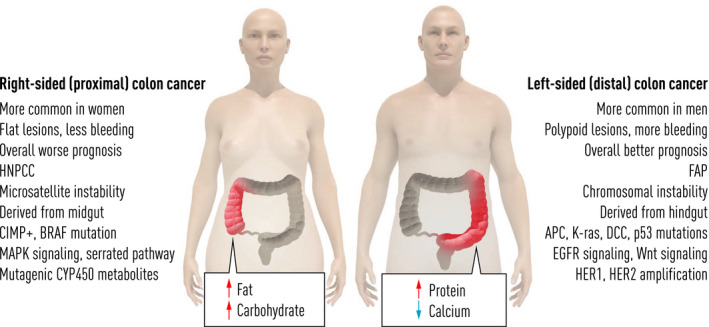
Colorectal cancer (CRC) is, besides breast, prostate, lung and skin cancers, the most common cancer worldwide and is suitable for screening. The incidence of CRC varies considerably in different parts of the world: in well-developed countries, the incidence is between 30 and 70 per 100 000 inhabitants, whereas in less-developed countries such as sub-Saharan Africa, it is 10-20/100 000 inhabitants. Women have a lower incidence of CRC, which is usually one-third of total incidence. Several studies have shown that it is possible to decrease mortality from CRC with about 20%, which is evidenced through the data from countries with screening programmes. Though the method of choice to identify blood samples in faecal matter is under debate, the most feasible way is to perform colonoscopy. Other methods include more advanced faecal analyses, testing for mutations from CRC, sigmoidoscopy, CT colonoscopy or optical colonoscopy. Colonoscopy is in most countries not available in sufficient amount and has to be carried out with great accuracy; otherwise, lesions will be missed to identify, thus leading to complications. Gender is an issue in CRC screening, as women have about 20% fewer colorectal adenomas and CRCs, but they also have more right-sided lesions, which are more difficult to detect with tests for faecal blood since they create less blood in faeces. Thus, other strategies may have to be developed for women in order for screening to have the same effect. It is essential to introduce colorectal cancer screening in all countries together with other clinical pieces of advice such as information on smoking, obesity and exercise in order to reduce one of the most dangerous cancers.
Keywords: F-Hb; colonoscopy; colorectal cancer; screening.
© 2020 The Authors. Journal of Internal Medicine published by John Wiley & Sons Ltd on behalf of Association for Publication of The Journal of Internal Medicine.
Conflict of interest statement
The author declares they have no conflict of interest.
Figures
References
-
- Ferlay J, Colombet M, Soerjomataram I et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer 2021; 144: 1941–53. - PubMed
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68: 394–424. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
