

Mechanisms of Cerebral Microbleeds
- PMID: 32930790
- PMCID: PMC7580489
- DOI: 10.1093/jnen/nlaa082
Mechanisms of Cerebral Microbleeds
Erratum in
-
Erratum to: Mechanisms of Cerebral Microbleeds.J Neuropathol Exp Neurol. 2021 Mar 22;80(4):388. doi: 10.1093/jnen/nlaa145. J Neuropathol Exp Neurol. 2021. PMID: 33463693 Free PMC article. No abstract available.
Abstract
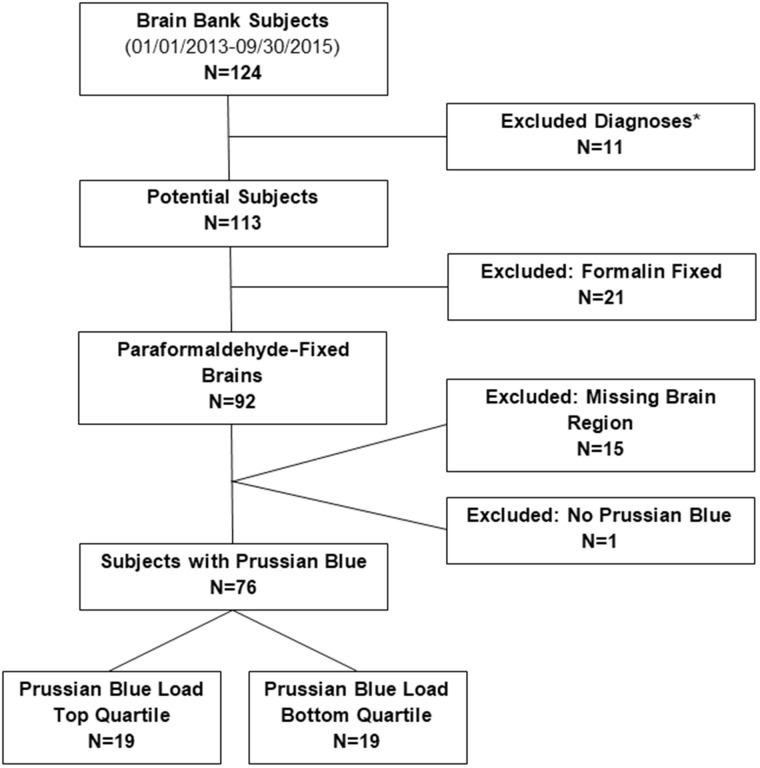
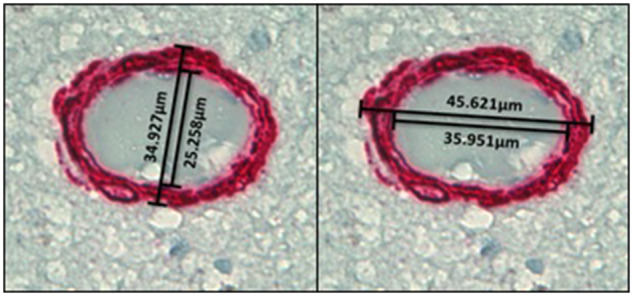
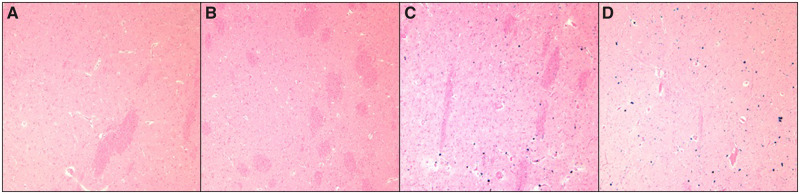
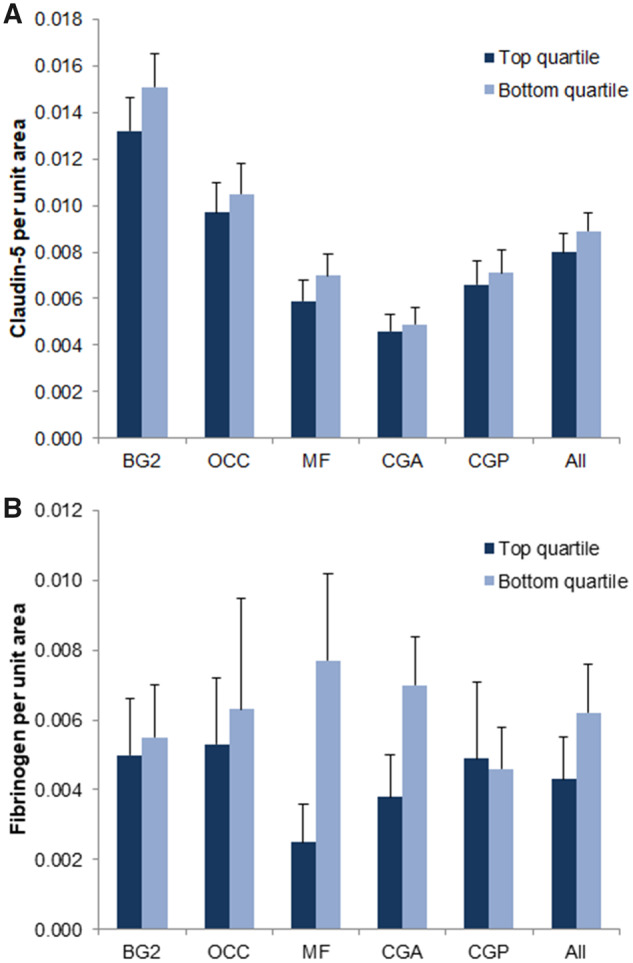
Cerebral microbleeds (CMB) are a common MRI finding, representing underlying cerebral microhemorrhages (CMH). The etiology of CMB and microhemorrhages is obscure. We conducted a pathological investigation of CMH, combining standard and immunohistological analyses of postmortem human brains. We analyzed 5 brain regions (middle frontal gyrus, occipital pole, rostral cingulate cortex, caudal cingulate cortex, and basal ganglia) of 76 brain bank subjects (mean age ± SE 90 ± 1.4 years). Prussian blue positivity, used as an index of CMH, was subjected to quantitative analysis for all 5 brain regions. Brains from the top and bottom quartiles (n = 19 each) were compared for quantitative immunohistological findings of smooth muscle actin, claudin-5, and fibrinogen, and for Sclerosis Index (SI) (a measure of arteriolar remodeling). Brains in the top quartile (i.e. with most extensive CMH) had significantly higher SI in the 5 brain regions combined (0.379 ± 0.007 vs 0.355 ± 0.008; p < 0.05). These findings indicate significant coexistence of arteriolar remodeling with CMH. While these findings provide clues to mechanisms of microhemorrhage development, further studies of experimental neuropathology are needed to determine causal relationships.
Keywords: Arteriosclerosis; Autopsy; Blood-brain barrier; Cerebral microhemorrhage; Histology; Immunohistochemistry.
© The Author(s) 2020. Published by Oxford University Press.
Figures

References
-
- Charidimou A, Krishnan A, Werring DJ, et al. Cerebral microbleeds: A guide to detection and clinical relevance in different disease settings. Neuroradiology 2013;55:655–74 - PubMed
-
- Kim TW, Lee SJ, Koo J, et al. Cerebral microbleeds and functional outcomes after ischemic stroke. Can J Neurol Sci 2014;41:577–82 - PubMed
-
- Bokura H, Saika R, Yamaguchi T, et al. Microbleeds are associated with subsequent hemorrhagic and ischemic stroke in healthy elderly individuals. Stroke 2011;42:1867–71 - PubMed
