

Survival in Patients With Brain Metastases: Summary Report on the Updated Diagnosis-Specific Graded Prognostic Assessment and Definition of the Eligibility Quotient
- PMID: 32931399
- PMCID: PMC7655019
- DOI: 10.1200/JCO.20.01255
Survival in Patients With Brain Metastases: Summary Report on the Updated Diagnosis-Specific Graded Prognostic Assessment and Definition of the Eligibility Quotient
Abstract
Purpose: Conventional wisdom has rendered patients with brain metastases ineligible for clinical trials for fear that poor survival could mask the benefit of otherwise promising treatments. Our group previously published the diagnosis-specific Graded Prognostic Assessment (GPA). Updates with larger contemporary cohorts using molecular markers and newly identified prognostic factors have been published. The purposes of this work are to present all the updated indices in a single report to guide treatment choice, stratify research, and define an eligibility quotient to expand eligibility.
Methods: A multi-institutional database of 6,984 patients with newly diagnosed brain metastases underwent multivariable analyses of prognostic factors and treatments associated with survival for each primary site. Significant factors were used to define the updated GPA. GPAs of 4.0 and 0.0 correlate with the best and worst prognoses, respectively.
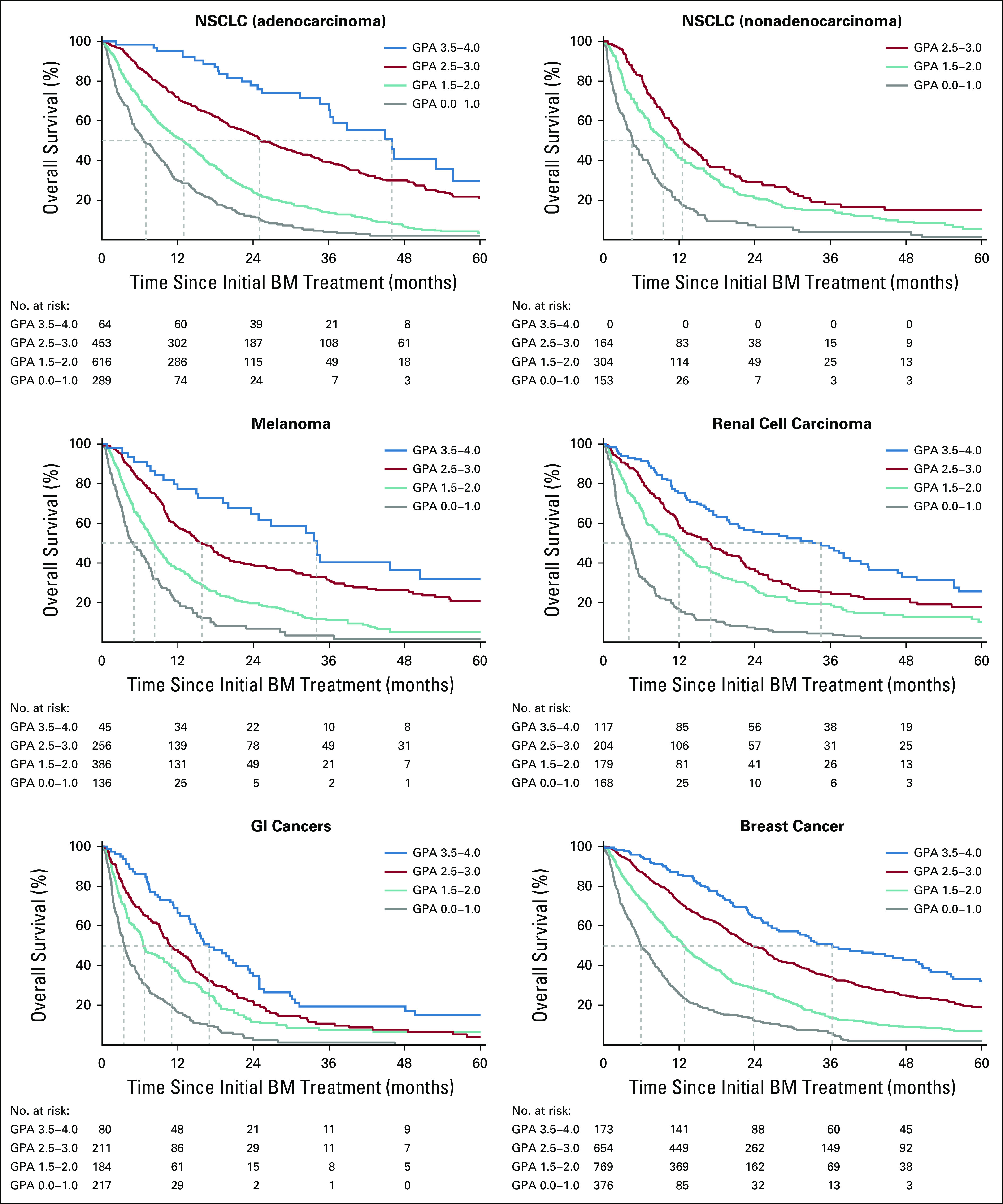
Results: Significant prognostic factors varied by diagnosis and new prognostic factors were identified. Those factors were incorporated into the updated GPA with robust separation (P < .01) between subgroups. Survival has improved, but varies widely by GPA for patients with non-small-cell lung, breast, melanoma, GI, and renal cancer with brain metastases from 7-47 months, 3-36 months, 5-34 months, 3-17 months, and 4-35 months, respectively.
Conclusion: Median survival varies widely and our ability to estimate survival for patients with brain metastases has improved. The updated GPA (available free at brainmetgpa.com) provides an accurate tool with which to estimate survival, individualize treatment, and stratify clinical trials. Instead of excluding patients with brain metastases, enrollment should be encouraged and those trials should be stratified by the GPA to ensure those trials make appropriate comparisons. Furthermore, we recommend the expansion of eligibility to allow for the enrollment of patients with previously treated brain metastases who have a 50% or greater probability of an additional year of survival (eligibility quotient > 0.50).
Figures
References
-
- Lin NU, Prowell T, Tan AR, et al. Modernizing clinical trial eligibility criteria: Recommendations of the American Society of Clinical Oncology-Friends of Cancer Research brain metastases working group. J Clin Oncol. 2017;35:3760–3773. - PubMed
-
- Harvey RD, Rubinstein WS, Ison G, et al. Impact of broadening clinical trial eligibility criteria for advanced non-small cell lung cancer patients: Real-world analysis. J Clin Oncol. 2019;37(suppl; abstr LBA108) - PubMed
-
- Gavrilovic IT, Posner JB. Brain metastases: Epidemiology and pathophysiology. J Neurooncol. 2005;75:5–14. - PubMed
