

The ABO histo-blood group, endothelial activation, and acute respiratory distress syndrome risk in critical illness
- PMID: 32931480
- PMCID: PMC7773362
- DOI: 10.1172/JCI139700
The ABO histo-blood group, endothelial activation, and acute respiratory distress syndrome risk in critical illness
Abstract
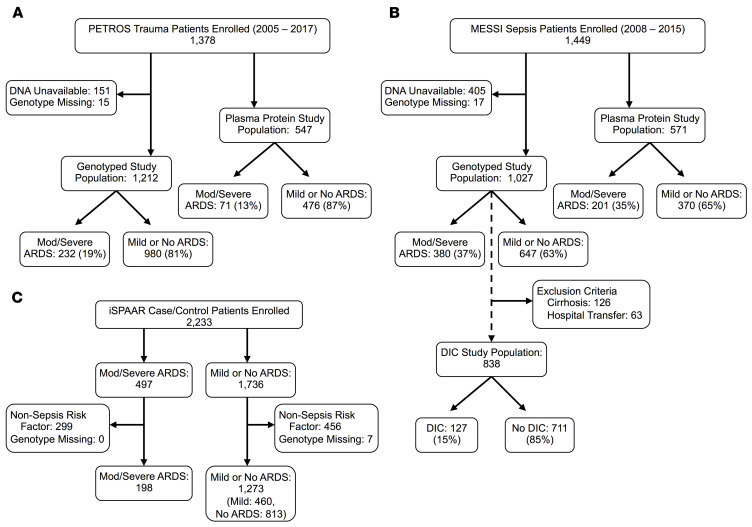
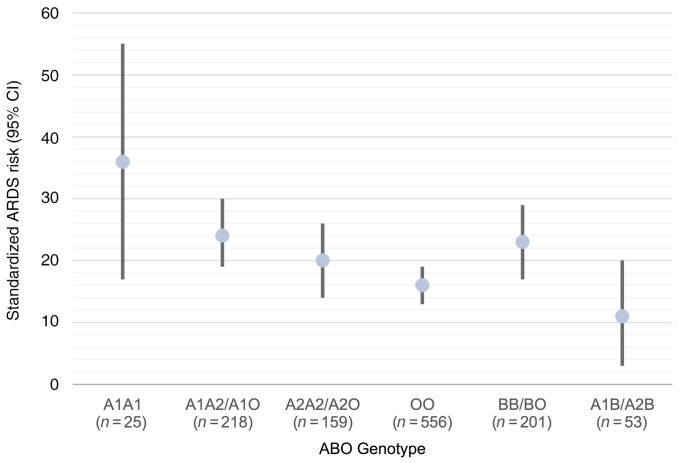
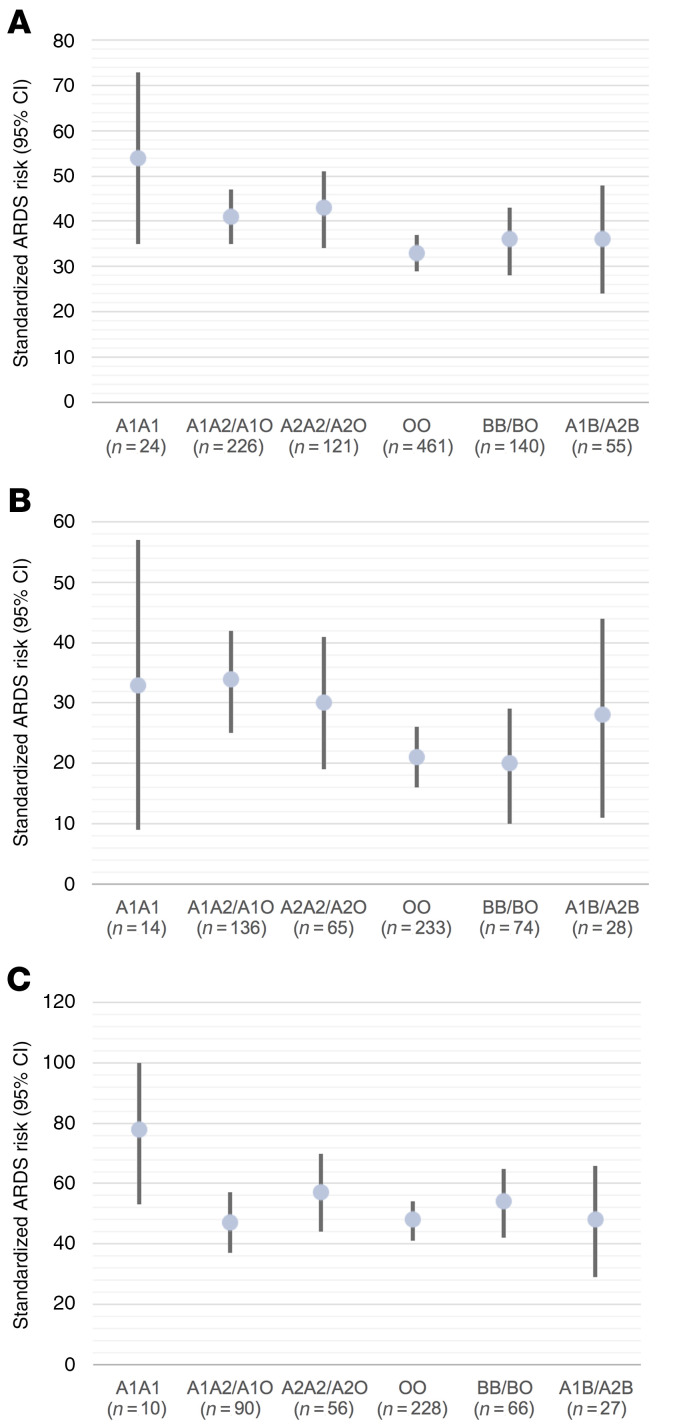
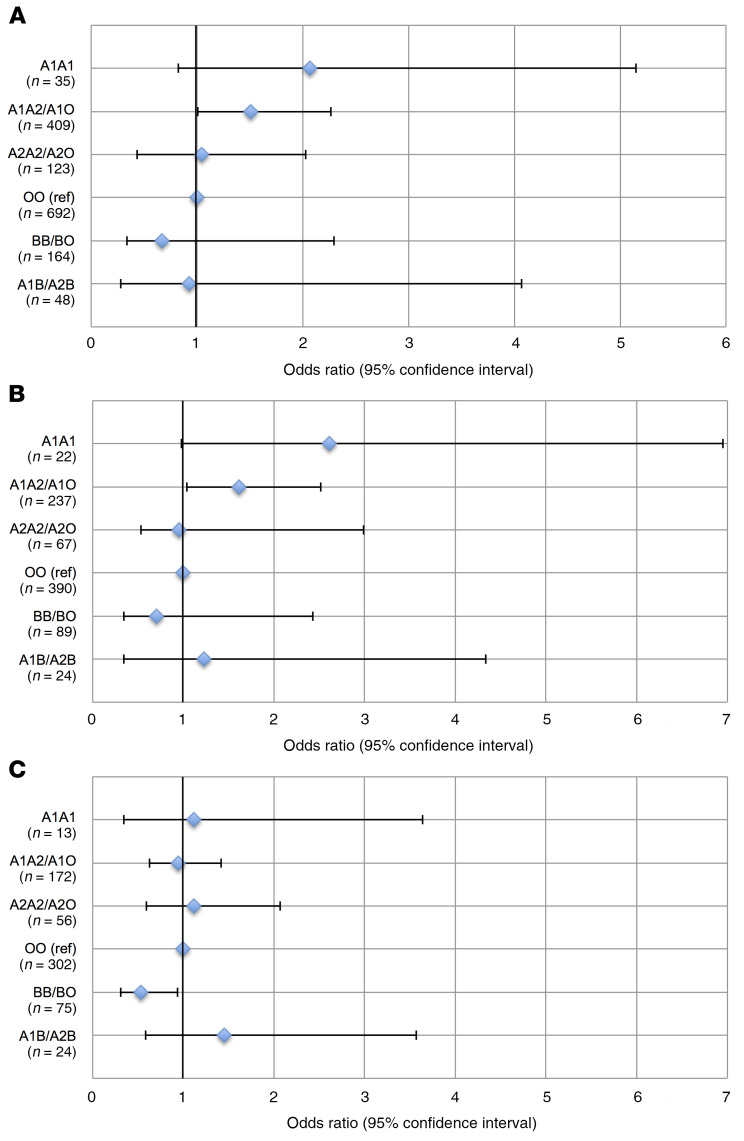
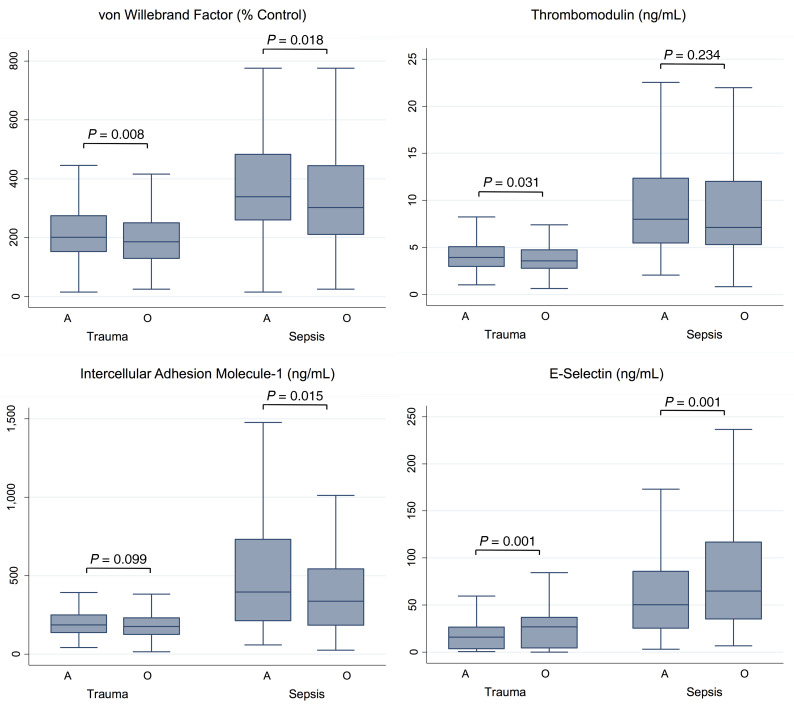
BACKGROUNDThe ABO histo-blood group is defined by carbohydrate modifications and is associated with risk for multiple diseases, including acute respiratory distress syndrome (ARDS). We hypothesized that genetically determined blood subtype A1 is associated with increased risk of ARDS and markers of microvascular dysfunction and coagulation.METHODSWe conducted analyses in 3 cohorts of critically ill trauma and sepsis patients (n = 3710) genotyped on genome-wide platforms to determine the association of the A1 blood type genotype with ARDS risk. We subsequently determined whether associations were present in FUT2-defined nonsecretors who lack ABO antigens on epithelium, but not endothelium. In a patient subgroup, we determined the associations of blood type with plasma levels of endothelial glycoproteins and disseminated intravascular coagulation (DIC). Lastly, we tested whether blood type A was associated with less donor lung injury recovery during human ex vivo lung perfusion (EVLP).RESULTSThe A1 genotype was associated with a higher risk of moderate to severe ARDS relative to type O in all 3 populations. In sepsis, this relationship was strongest in nonpulmonary infections. The association persisted in nonsecretors, suggesting a vascular mechanism. The A1 genotype was also associated with higher DIC risk as well as concentrations of thrombomodulin and von Willebrand factor, which in turn were associated with ARDS risk. Blood type A was also associated with less lung injury recovery during EVLP.CONCLUSIONWe identified a replicable association between ABO blood type A1 and risk of ARDS among the critically ill, possibly mediated through microvascular dysfunction and coagulation.FUNDINGNIH HL122075, HL125723, HL137006, HL137915, DK097307, HL115354, HL101779, and the University of Pennsylvania McCabe Fund Fellowship Award.
Keywords: Coagulation; Epidemiology; Pulmonology; endothelial cells.
Conflict of interest statement
Figures
Comment in
-
ABO blood type: a window into the genetics of acute respiratory distress syndrome susceptibility.J Clin Invest. 2021 Jan 4;131(1):e144075. doi: 10.1172/JCI144075. J Clin Invest. 2021. PMID: 33141764 Free PMC article.
References
-
- The ARDS Definition Task Force, et al. Acute respiratory distress syndrome: the Berlin definition. JAMA. 2012;307(23):2526–2533. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
