

Modulating the tension-time integral of the cardiac twitch prevents dilated cardiomyopathy in murine hearts
- PMID: 32931484
- PMCID: PMC7605524
- DOI: 10.1172/jci.insight.142446
Modulating the tension-time integral of the cardiac twitch prevents dilated cardiomyopathy in murine hearts
Abstract
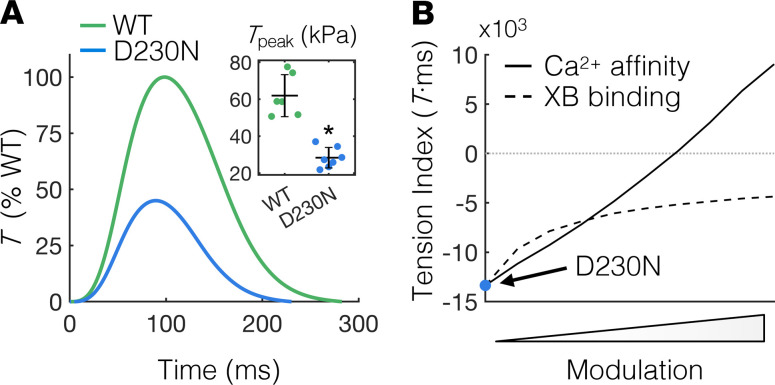
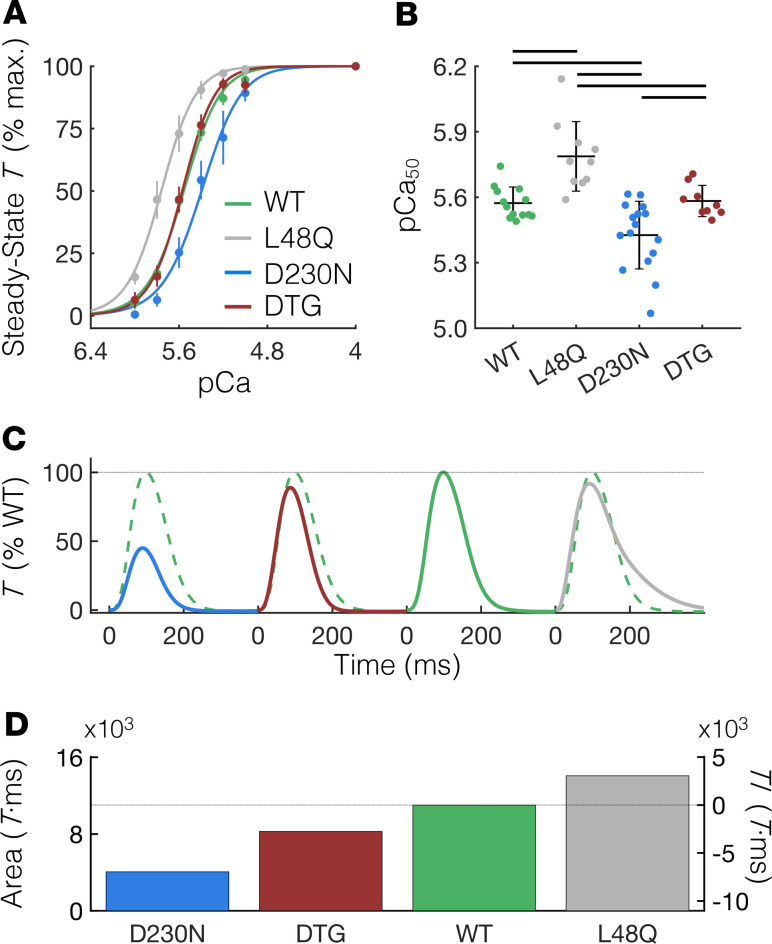
Dilated cardiomyopathy (DCM) is often associated with sarcomere protein mutations that confer reduced myofilament tension-generating capacity. We demonstrated that cardiac twitch tension-time integrals can be targeted and tuned to prevent DCM remodeling in hearts with contractile dysfunction. We employed a transgenic murine model of DCM caused by the D230N-tropomyosin (Tm) mutation and designed a sarcomere-based intervention specifically targeting the twitch tension-time integral of D230N-Tm hearts using multiscale computational models of intramolecular and intermolecular interactions in the thin filament and cell-level contractile simulations. Our models predicted that increasing the calcium sensitivity of thin filament activation using the cardiac troponin C (cTnC) variant L48Q can sufficiently augment twitch tension-time integrals of D230N-Tm hearts. Indeed, cardiac muscle isolated from double-transgenic hearts expressing D230N-Tm and L48Q cTnC had increased calcium sensitivity of tension development and increased twitch tension-time integrals compared with preparations from hearts with D230N-Tm alone. Longitudinal echocardiographic measurements revealed that DTG hearts retained normal cardiac morphology and function, whereas D230N-Tm hearts developed progressive DCM. We present a computational and experimental framework for targeting molecular mechanisms governing the twitch tension of cardiomyopathic hearts to counteract putative mechanical drivers of adverse remodeling and open possibilities for tension-based treatments of genetic cardiomyopathies.
Keywords: Cardiology; Cardiovascular disease; Molecular pathology.
Conflict of interest statement
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
- RM1 GM131981/GM/NIGMS NIH HHS/United States
- T32 EB001650/EB/NIBIB NIH HHS/United States
- K08 HL128826/HL/NHLBI NIH HHS/United States
- T32 HL105373/HL/NHLBI NIH HHS/United States
- R01 HL137100/HL/NHLBI NIH HHS/United States
- T32 HL007444/HL/NHLBI NIH HHS/United States
- F32 HL152573/HL/NHLBI NIH HHS/United States
- R01 HL107046/HL/NHLBI NIH HHS/United States
- P30 AR074990/AR/NIAMS NIH HHS/United States
- U01 HL122199/HL/NHLBI NIH HHS/United States
- T32 HL007312/HL/NHLBI NIH HHS/United States
- R01 HL141187/HL/NHLBI NIH HHS/United States
- R01 HL142624/HL/NHLBI NIH HHS/United States
- R01 HL128368/HL/NHLBI NIH HHS/United States
- R01 HL075619/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
