

Impact of the COVID-19 Pandemic on Surgical Training and Learner Well-Being: Report of a Survey of General Surgery and Other Surgical Specialty Educators
- PMID: 32931914
- PMCID: PMC7486868
- DOI: 10.1016/j.jamcollsurg.2020.08.766
Impact of the COVID-19 Pandemic on Surgical Training and Learner Well-Being: Report of a Survey of General Surgery and Other Surgical Specialty Educators
Abstract
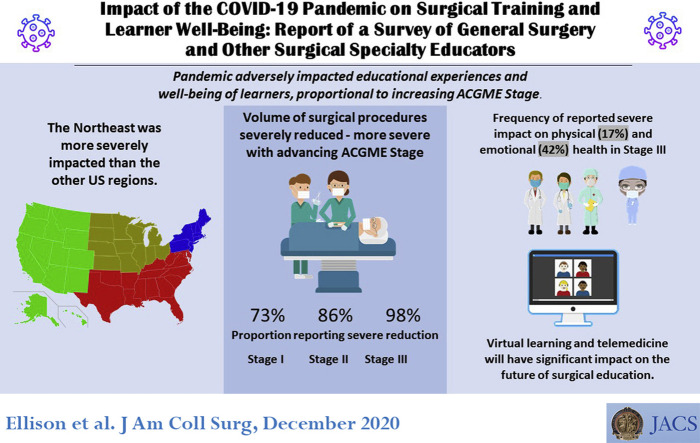
Background: The COVID-19 pandemic disrupted the delivery of surgical services. The purpose of this communication was to report the impact of the pandemic on surgical training and learner well-being and to document adaptations made by surgery departments.
Study design: A 37-item survey was distributed to educational leaders in general surgery and other surgical specialty training programs. It included both closed- and open-ended questions and the self-reported stages of GME during the COVID-19 pandemic, as defined by the ACGME. Statistical associations for items with stage were assessed using categorical analysis.
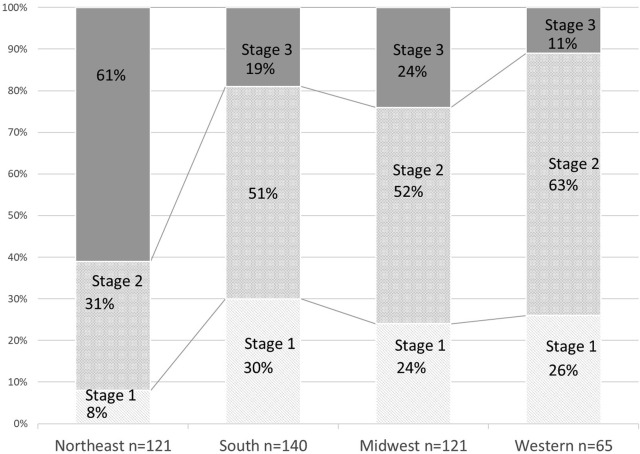
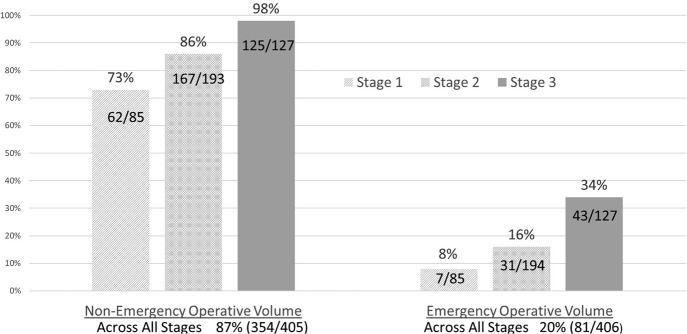
Results: The response rate was 21% (472 of 2,196). US stage distribution (n = 447) was as follows: stage 1, 22%; stage 2, 48%; and stage 3, 30%. Impact on clinical education significantly increased by stage, with severe reductions in nonemergency operations (73% and 86% vs 98%) and emergency operations (8% and 16% vs 34%). Variable effects were reported on minimal expected case numbers across all stages. Reductions were reported in outpatient experience (83%), in-hospital experience (70%), and outside rotations (57%). Increases in ICU rotations were reported with advancing stage (7% and 13% vs 37%). Severity of impact on didactic education increased with stage (14% and 30% vs 46%). Virtual conferences were adopted by 97% across all stages. Severity of impact on learner well-being increased by stage-physical safety (6% and 9% vs 31%), physical health (0% and 7% vs 17%), and emotional health (11% and 24% vs 42%). Regardless of stage, most but not all made adaptations to support trainees' well-being.
Conclusions: The pandemic adversely impacted surgical training and the well-being of learners across all surgical specialties proportional to increasing ACGME stage. There is a need to develop education disaster plans to support technical competency and learner well-being. Careful assessment for program advancement will also be necessary. The experience during this pandemic shows that virtual learning and telemedicine will have a considerable impact on the future of surgical education.
Copyright © 2020 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Educational and Training Lessons from the COVID-19 Pandemic: We Must Prepare for the Next Pandemic.J Am Coll Surg. 2020 Dec;231(6):626-627. doi: 10.1016/j.jamcollsurg.2020.09.003. J Am Coll Surg. 2020. PMID: 33243393 Free PMC article. No abstract available.
References
-
- Hoxsey R., Smith M., Miller J., Nolan T. Surviving disaster: assessment of obstetrics and gynecology training at Louisiana State University-New Orleans before and after Hurricane Katrina. Am J Med Sci. 2008;336:151–155. - PubMed
