

Higher Adenoma Detection Rates at Screening Associated With Lower Long-Term Colorectal Cancer Incidence and Mortality
- PMID: 32931959
- PMCID: PMC8811539
- DOI: 10.1016/j.cgh.2020.09.020
Higher Adenoma Detection Rates at Screening Associated With Lower Long-Term Colorectal Cancer Incidence and Mortality
Abstract
Background & aims: Detection and removal of adenomas reduces colorectal cancer (CRC) risk. The impact of adenoma detection rates (ADRs) on long-term CRC incidence and mortality is unknown. We investigated this using data from the UK Flexible Sigmoidoscopy Screening Trial.
Methods: Of 167,882 UK Flexible Sigmoidoscopy Screening Trial participants, 40,085 were in the intervention arm and underwent flexible sigmoidoscopy screening at 13 trial centers. The median follow-up time was 17 years. At each center, 1 endoscopist performed most flexible sigmoidoscopies. Multivariable logistic regression was used to classify centers into high-, intermediate-, and low-detector groups based on their main endoscopist's ADR. We calculated the incidence and mortality of distal and all-site CRC, and estimated hazard ratios (HRs) with 95% CIs using Cox regression.
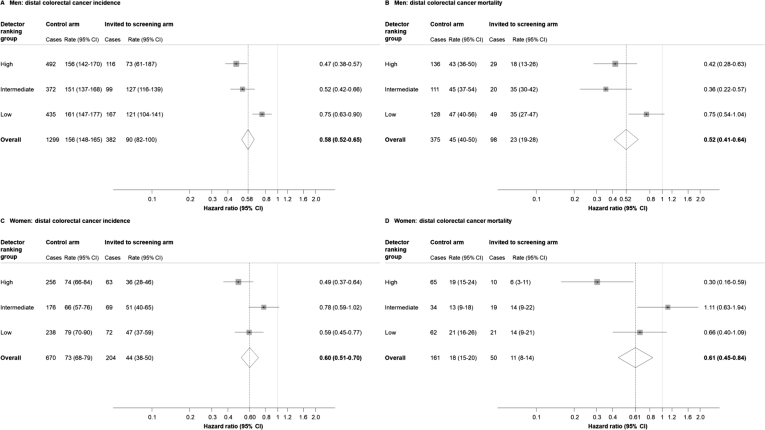
Results: Five, 4, and 4 centers, respectively, were classified into the high-detector, intermediate-detector, and low-detector groups. The average ADRs in each respective group were 15%, 12%, and 9%. Distal CRC incidence and mortality were reduced among those screened compared with controls in all groups, and effects of screening varied significantly by detector ranking, with larger reductions in incidence and mortality seen in the high-detector group (incidence: HR, 0.34; 95% CI, 0.27-0.42; mortality: HR, 0.22, 95% CI, 0.13-0.37) than in the low-detector group (incidence: HR, 0.55; 95% CI, 0.44-0.68; mortality: HR, 0.54; 95% CI, 0.34-0.86). Similar results were observed for all-site CRC, with larger effects seen in the high-detector (incidence: HR, 0.58; 95% CI, 0.50-0.67; mortality: HR, 0.52; 95% CI, 0.39-0.69) than in the low-detector group (incidence: HR, 0.72; 95% CI, 0.61-0.85; mortality: HR, 0.68; 95% CI, 0.51-0.92), although the heterogeneity was not statistically significant.
Conclusions: Higher ADRs at screening provide greater long-term protection against CRC incidence and mortality. Isrctn.org, number: ISRCTN28352761.
Keywords: Adenoma Detection Rate; Colorectal Cancer; Flexible Sigmoidoscopy; Screening.
Copyright © 2022 The Authors. Published by Elsevier Inc. All rights reserved.
Figures







Comment in
-
Adenoma Detection Rate: The Gift That Keeps on Giving.Clin Gastroenterol Hepatol. 2022 Feb;20(2):e25-e27. doi: 10.1016/j.cgh.2020.11.003. Epub 2020 Nov 3. Clin Gastroenterol Hepatol. 2022. PMID: 33157319 No abstract available.
References
-
- Levin B., Lieberman D.A., McFarland B., et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology. 2008;134:1570–1595. - PubMed
-
- Atkin W.S., Edwards R., Kralj-Hans I., et al. Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicentre randomised controlled trial. Lancet. 2010;375:1624–1633. - PubMed
-
- Mayor S. UK committee recommends flexible sigmoidoscopy to screen for bowel cancer. BMJ. 2011:342.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
