

Prognostic value of tertiary lymphoid structure and tumour infiltrating lymphocytes in oral squamous cell carcinoma
- PMID: 32934197
- PMCID: PMC7493903
- DOI: 10.1038/s41368-020-00092-3
Prognostic value of tertiary lymphoid structure and tumour infiltrating lymphocytes in oral squamous cell carcinoma
Abstract
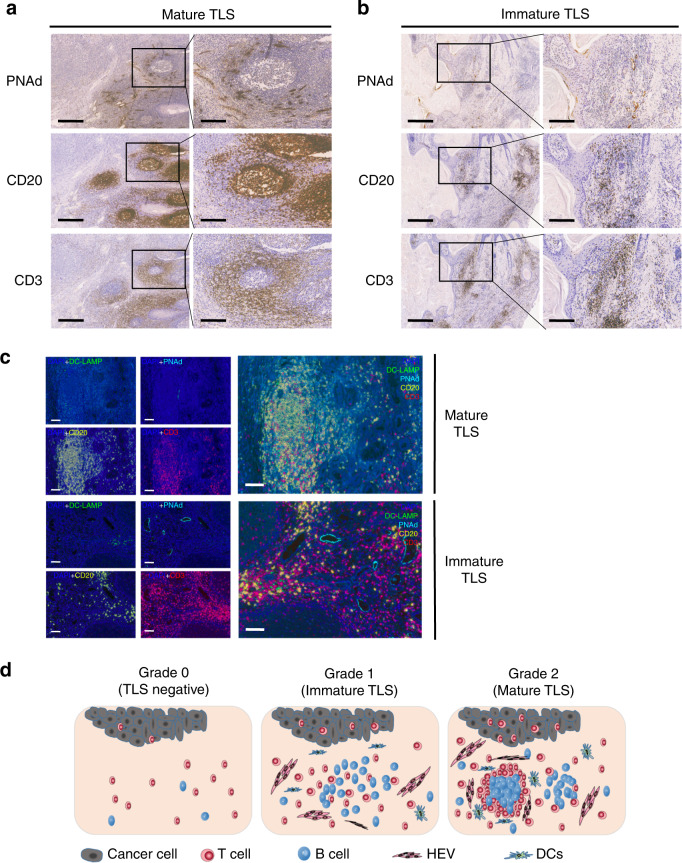
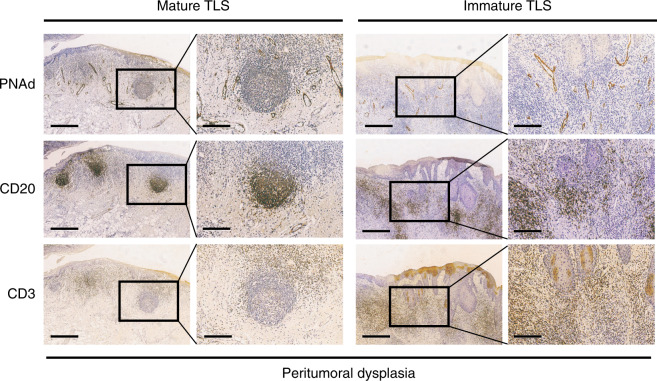
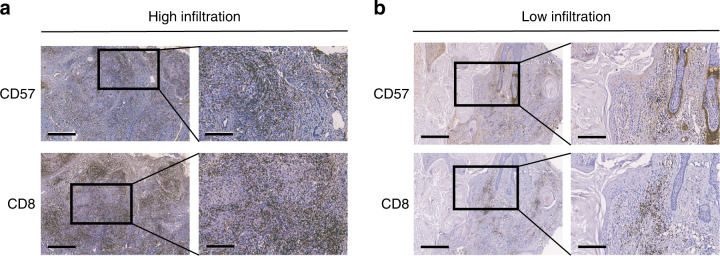
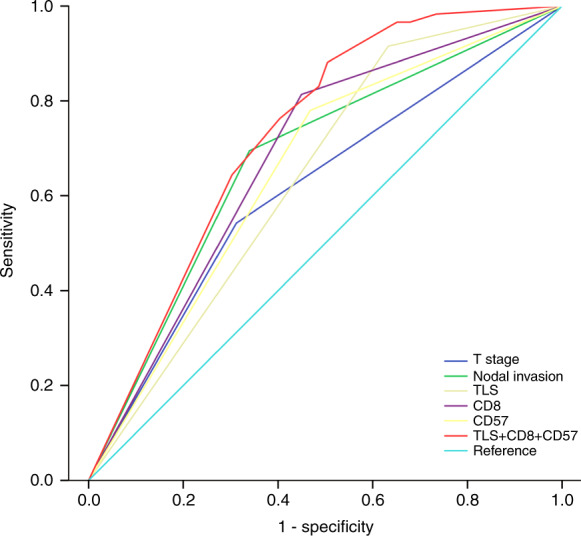
Tertiary lymphoid structures (TLS) are ectopic lymphoid structures in cancers that are largely associated with favourable prognosis. However, the prognostic value of TLSs in oral squamous cell carcinoma (OSCC) is largely unknown, and the association between tumour infiltrating lymphocytes (TILs) and TLSs has been rarely explored in OSCC. In this study, associated markers of TLS, including peripheral node address (PNAd) in high endothelial venules, CD20 in B cells and CD3 in T cells, were examined in 168 OSCC patients, and survival analysis was performed between TLS-positive and TLS-negative cohorts. We detected the presence of TILs by staining CD8+ cytotoxic T cells and CD57+ NK cells as well. TLSs appeared as highly organized structures in 45 (26.8%) cases. TLS-positive patients had a better 5-year overall survival (OS) rate (88.9% vs. 56.1%, P < 0.001) and relapse-free survival (RFS) rate (88.9% vs. 63.4%, P = 0.002). Moreover, the presence of TLS was an independent prognostic factor for both the 5-year OS rate (hazard ratio [HR] = 3.784; 95% confidence interval [CI], 1.498-9.562) and RFS rate (HR = 3.296; 95% CI, 1.279-8.490) in multivariate analysis. Furthermore, a higher density of CD8+ T cells and CD57+ NK cells was found in TLS-positive sections than in TLS-negative counterparts (P < 0.001), and their combination provided a higher predictive accuracy (AUC = 0.730; 95% CI, 0.654-0.805). In conclusion, our results suggest that TLS is an independent positive prognostic factor for OSCC patients. These findings provide a theoretical basis for the future diagnostic and therapeutic value of TLSs in OSCC treatment.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Bray F, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018;68:394–424. - PubMed
-
- Chi AC, Day TA, Neville BW. Oral cavity and oropharyngeal squamous cell carcinoma–an update. CA Cancer J. Clin. 2015;65:401–421. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J. Clin. 2020;70:7–30. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
