

Neuropathological correlates of cortical superficial siderosis in cerebral amyloid angiopathy
- PMID: 32935842
- PMCID: PMC8453293
- DOI: 10.1093/brain/awaa266
Neuropathological correlates of cortical superficial siderosis in cerebral amyloid angiopathy
Abstract
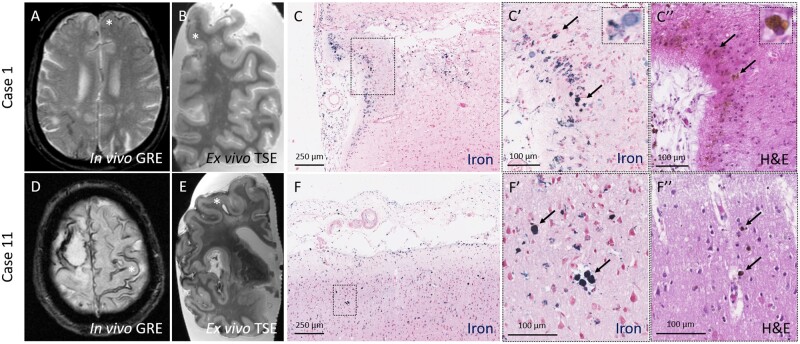
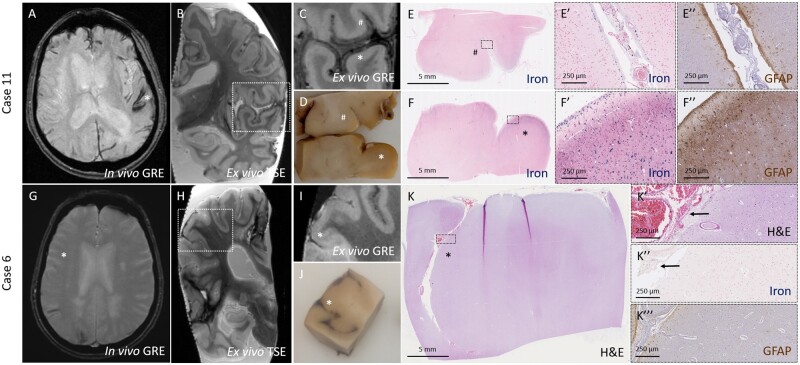
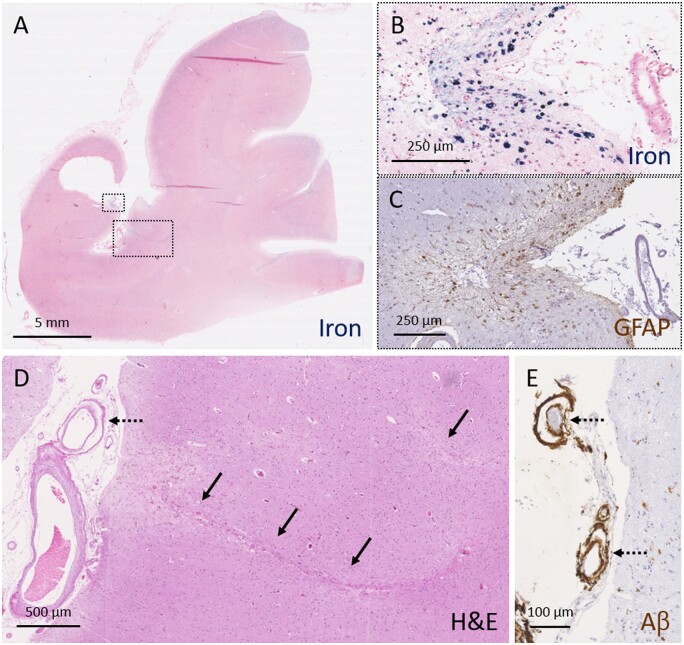
Cortical superficial siderosis is an established haemorrhagic neuroimaging marker of cerebral amyloid angiopathy. In fact, cortical superficial siderosis is emerging as a strong independent risk factor for future lobar intracerebral haemorrhage. However, the underlying neuropathological correlates and pathophysiological mechanisms of cortical superficial siderosis remain elusive. Here we use an in vivo MRI, ex vivo MRI, histopathology approach to assess the neuropathological correlates and vascular pathology underlying cortical superficial siderosis. Fourteen autopsy cases with cerebral amyloid angiopathy (mean age at death 73 years, nine males) and three controls (mean age at death 91 years, one male) were included in the study. Intact formalin-fixed cerebral hemispheres were scanned on a 3 T MRI scanner. Cortical superficial siderosis was assessed on ex vivo gradient echo and turbo spin echo MRI sequences and compared to findings on available in vivo MRI. Subsequently, 11 representative areas in four cases with available in vivo MRI scans were sampled for histopathological verification of MRI-defined cortical superficial siderosis. In addition, samples were taken from predefined standard areas of the brain, blinded to MRI findings. Serial sections were stained for haematoxylin and eosin and Perls' Prussian blue, and immunohistochemistry was performed against amyloid-β and GFAP. Cortical superficial siderosis was present on ex vivo MRI in 8/14 cases (57%) and 0/3 controls (P = 0.072). Histopathologically, cortical superficial siderosis corresponded to iron-positive haemosiderin deposits in the subarachnoid space and superficial cortical layers, indicative of chronic bleeding events originating from the leptomeningeal vessels. Increased severity of cortical superficial siderosis was associated with upregulation of reactive astrocytes. Next, cortical superficial siderosis was assessed on a total of 65 Perls'-stained sections from MRI-targeted and untargeted sampling combined in cerebral amyloid angiopathy cases. Moderate-to-severe cortical superficial siderosis was associated with concentric splitting of the vessel wall (an advanced form of cerebral amyloid angiopathy-related vascular damage) in leptomeningeal vessels (P < 0.0001), but reduced cerebral amyloid angiopathy severity in cortical vessels (P = 0.048). In terms of secondary tissue injury, moderate-to-severe cortical superficial siderosis was associated with the presence of microinfarcts (P = 0.025), though not microbleeds (P = 0.973). Collectively, these data suggest that cortical superficial siderosis on MRI corresponds to iron-positive deposits in the superficial cortical layers, representing the chronic manifestation of bleeding episodes from leptomeningeal vessels. Cortical superficial siderosis appears to be the result of predominantly advanced cerebral amyloid angiopathy of the leptomeningeal vessels and may trigger secondary ischaemic injury in affected areas.
Keywords: cerebral amyloid angiopathy; cortical superficial siderosis; magnetic resonance imaging; microbleeds; microinfarcts.
© The Author(s) (2020). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Charidimou A, Baron JC, Werring DJ. Cerebral amyloid angiopathy and transient focal neurological episodes. Cerebrovasc Dis 2013. b; 36: 245–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
