

Association of Clinical and Demographic Factors With the Severity of Palmoplantar Pustulosis
- PMID: 32936291
- PMCID: PMC7495329
- DOI: 10.1001/jamadermatol.2020.3275
Association of Clinical and Demographic Factors With the Severity of Palmoplantar Pustulosis
Abstract
Importance: Although palmoplantar pustulosis (PPP) can significantly impact quality of life, the factors underlying disease severity have not been studied.
Objective: To examine the factors associated with PPP severity.
Design, setting, and participants: An observational, cross-sectional study of 2 cohorts was conducted. A UK data set including 203 patients was obtained through the Anakinra in Pustular Psoriasis, Response in a Controlled Trial (2016-2019) and its sister research study Pustular Psoriasis, Elucidating Underlying Mechanisms (2016-2020). A Northern European cohort including 193 patients was independently ascertained by the European Rare and Severe Psoriasis Expert Network (2014-2017). Patients had been recruited in secondary or tertiary dermatology referral centers. All patients were of European descent. The PPP diagnosis was established by dermatologists, based on clinical examination and/or published consensus criteria. The present study was conducted from October 1, 2014, to March 15, 2020.
Main outcomes and measures: Demographic characteristics, comorbidities, smoking status, Palmoplantar Pustulosis Psoriasis Area Severity Index (PPPASI), measuring severity from 0 (no sign of disease) to 72 (very severe disease), or Physician Global Assessment (PGA), measuring severity as 0 (clear), 1 (almost clear), 2 (mild), 3 (moderate), and 4 (severe).
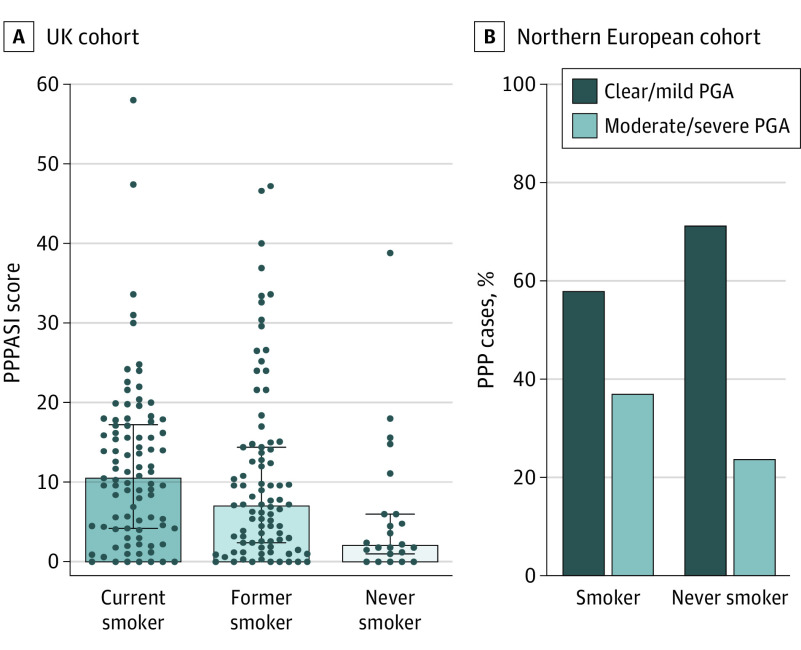
Results: Among the 203 UK patients (43 men [21%], 160 women [79%]; median age at onset, 48 [interquartile range (IQR), 38-59] years), the PPPASI was inversely correlated with age of onset (r = -0.18, P = .01). Similarly, in the 159 Northern European patients who were eligible for inclusion in this analysis (25 men [16%], 134 women [84%]; median age at onset, 45 [IQR, 34-53.3] years), the median age at onset was lower in individuals with a moderate to severe PGA score (41 years [IQR, 30.5-52 years]) compared with those with a clear to mild PGA score (46.5 years [IQR, 35-55 years]) (P = .04). In the UK sample, the median PPPASI score was higher in women (9.6 [IQR, 3.0-16.2]) vs men (4.0 [IQR, 1.0-11.7]) (P = .01). Likewise, moderate to severe PPP was more prevalent among Northern European women (57 of 134 [43%]) compared with men (5 of 25 [20%]) (P = .03). In the UK cohort, the median PPPASI score was increased in current smokers (10.7 [IQR, 4.2-17.5]) compared with former smokers (7 [IQR, 2.0-14.4]) and nonsmokers (2.2 [IQR, 1-6]) (P = .003). Comparable differences were observed in the Northern European data set, as the prevalence of moderate to severe PPP was higher in former and current smokers (51 of 130 [39%]) compared with nonsmokers (6 of 24 [25%]) (P = .14).
Conclusions and relevance: The findings of this study suggest that PPP severity is associated with early-onset disease, female sex, and smoking status. Thus, smoking cessation intervention might be beneficial.
Conflict of interest statement
Figures


References
-
- Mahil SK, Barker JN, Capon F. Pustular forms of psoriasis related to autoinflammation. In: Hashkes P, Laxer R, Simon A, eds. Textbook of Autoinflammation. Switzerland: Springer Nature; 2019:471-484. doi: 10.1007/978-3-319-98605-0_26 - DOI
-
- Wilsmann-Theis D, Jacobi A, Frambach Y, et al. Palmoplantar pustulosis—a cross-sectional analysis in Germany. Dermatol Online J. 2017;23(4):13030/qt0h15613d. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
