

Prognosticating Outcomes and Nudging Decisions with Electronic Records in the Intensive Care Unit Trial Protocol
- PMID: 32936675
- PMCID: PMC8020719
- DOI: 10.1513/AnnalsATS.202002-088SD
Prognosticating Outcomes and Nudging Decisions with Electronic Records in the Intensive Care Unit Trial Protocol
Abstract
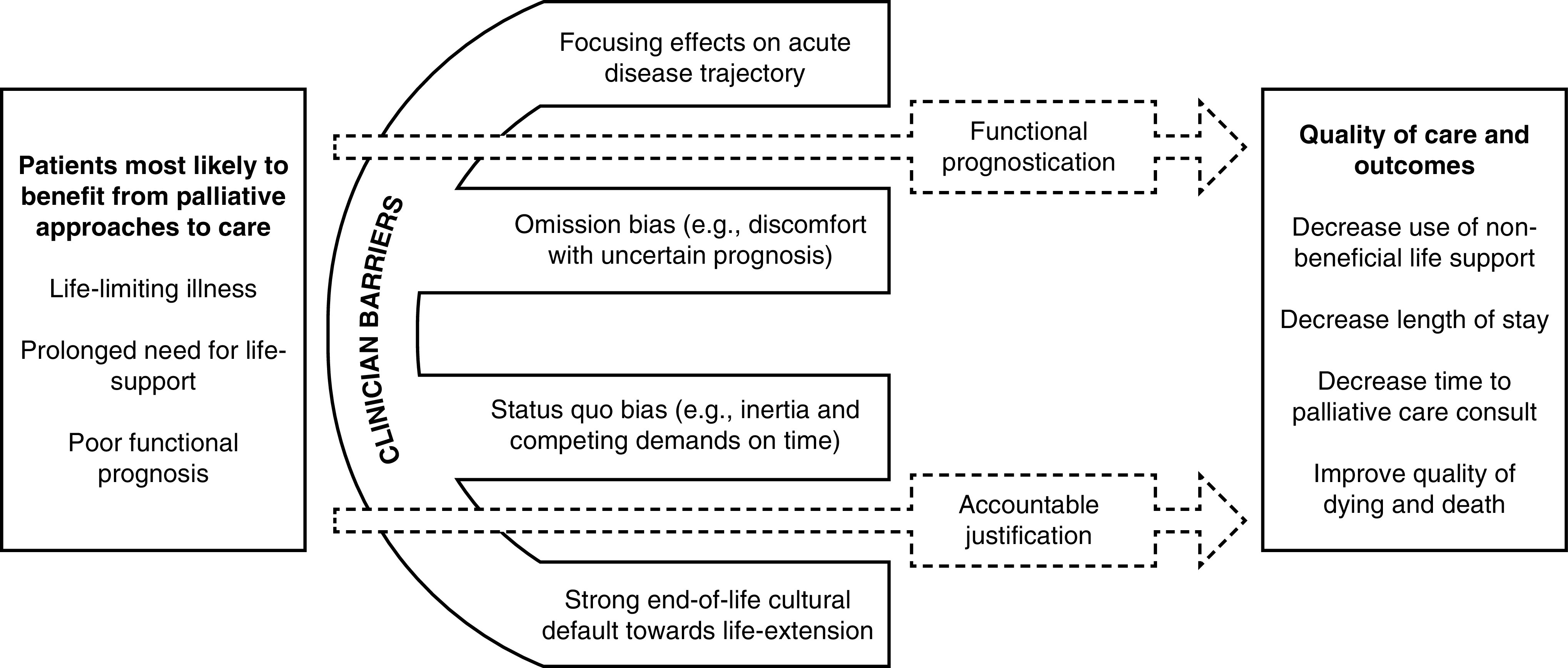
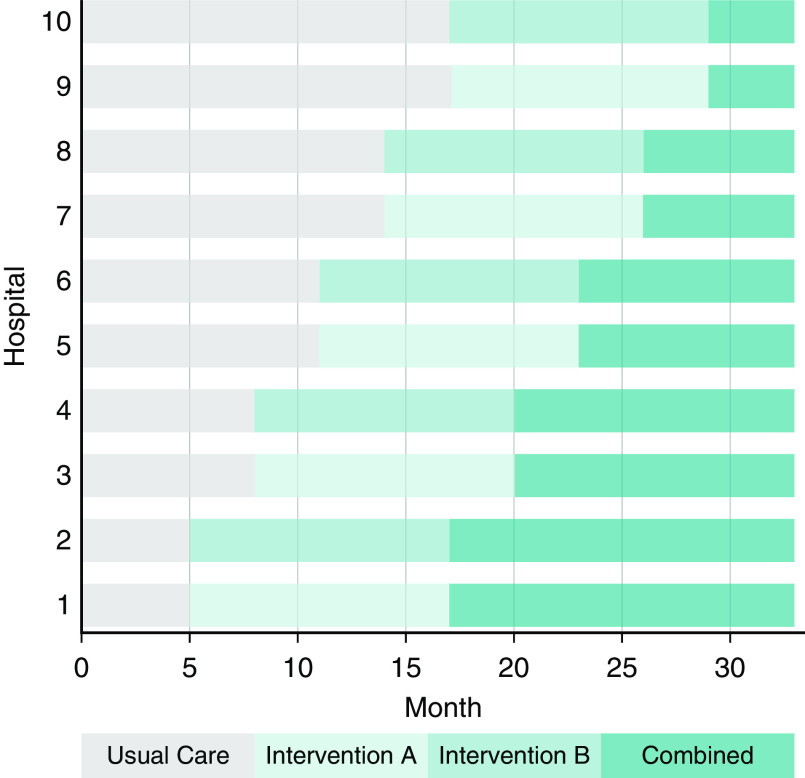
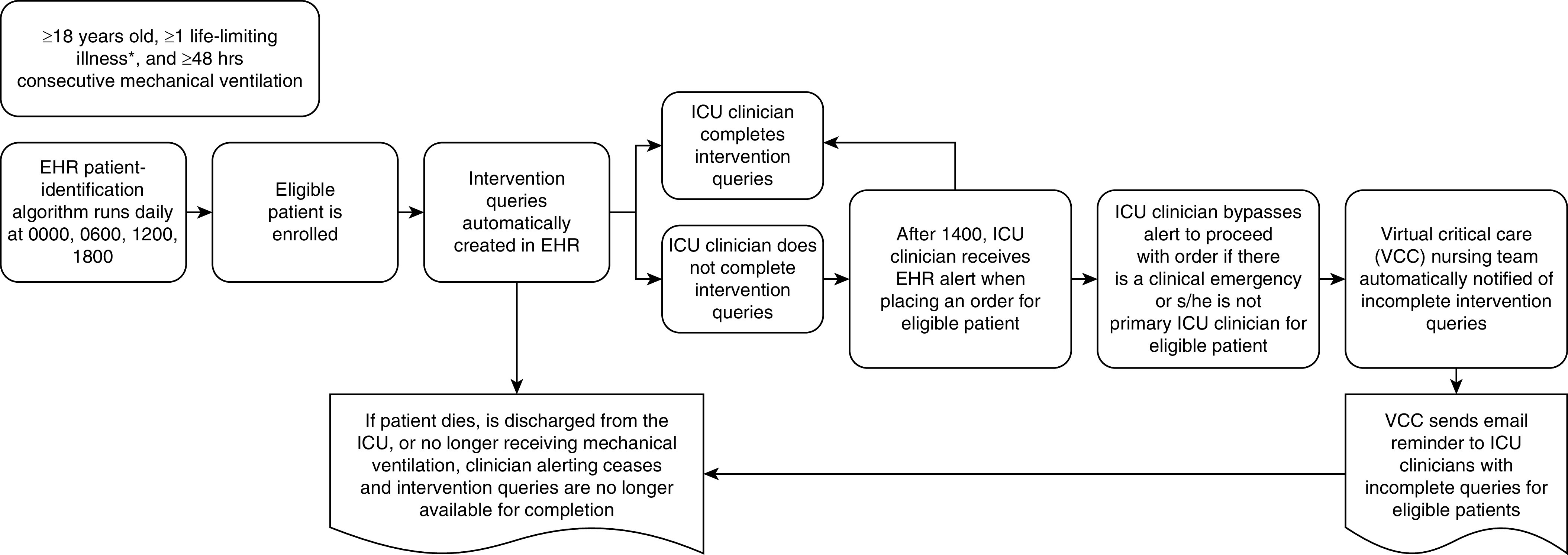
Expert recommendations to discuss prognosis and offer palliative options for critically ill patients at high risk of death are variably heeded by intensive care unit (ICU) clinicians. How to best promote such communication to avoid potentially unwanted aggressive care is unknown. The PONDER-ICU (Prognosticating Outcomes and Nudging Decisions with Electronic Records in the ICU) study is a 33-month pragmatic, stepped-wedge cluster randomized trial testing the effectiveness of two electronic health record (EHR) interventions designed to increase ICU clinicians' engagement of critically ill patients at high risk of death and their caregivers in discussions about all treatment options, including care focused on comfort. We hypothesize that the quality of care and patient-centered outcomes can be improved by requiring ICU clinicians to document a functional prognostic estimate (intervention A) and/or to provide justification if they have not offered patients the option of comfort-focused care (intervention B). The trial enrolls all adult patients admitted to 17 ICUs in 10 hospitals in North Carolina with a preexisting life-limiting illness and acute respiratory failure requiring continuous mechanical ventilation for at least 48 hours. Eligibility is determined using a validated algorithm in the EHR. The sequence in which hospitals transition from usual care (control), to intervention A or B and then to combined interventions A + B, is randomly assigned. The primary outcome is hospital length of stay. Secondary outcomes include other clinical outcomes, palliative care process measures, and nurse-assessed quality of dying and death.Clinical trial registered with clinicaltrials.gov (NCT03139838).
Keywords: artificial respiration; clinical trial; critical care; palliative care.
Figures
References
-
- Angus DC, Barnato AE, Linde-Zwirble WT, Weissfeld LA, Watson RS, Rickert T, et al. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med. 2004;32:638–643. - PubMed
-
- Kwok AC, Semel ME, Lipsitz SR, Bader AM, Barnato AE, Gawande AA, et al. The intensity and variation of surgical care at the end of life: a retrospective cohort study. Lancet. 2011;378:1408–1413. - PubMed
-
- Committee on Care at the End of Life, Institute of Medicine Fields MJ, Cassel CK.editors. Approaching death, improving care at the end of life Washington, DC: National Academy Press; 1997
-
- People’s memo to politicians: this is not your fight Time Magazine 2005 April 4 [accessed 2016 Jul 26]. Available from: http://content.time.com/time/magazine/article/0,9171,1042447,00.html
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
