

Subclinical Tuberculosis Disease-A Review and Analysis of Prevalence Surveys to Inform Definitions, Burden, Associations, and Screening Methodology
- PMID: 32936877
- PMCID: PMC8326537
- DOI: 10.1093/cid/ciaa1402
Subclinical Tuberculosis Disease-A Review and Analysis of Prevalence Surveys to Inform Definitions, Burden, Associations, and Screening Methodology
Abstract
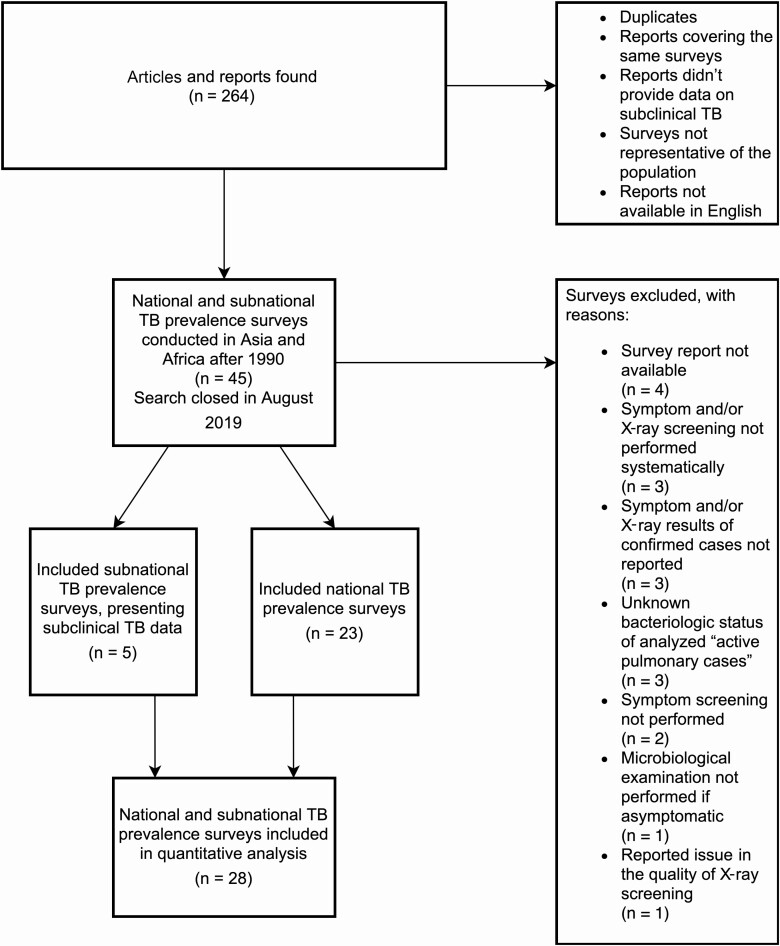
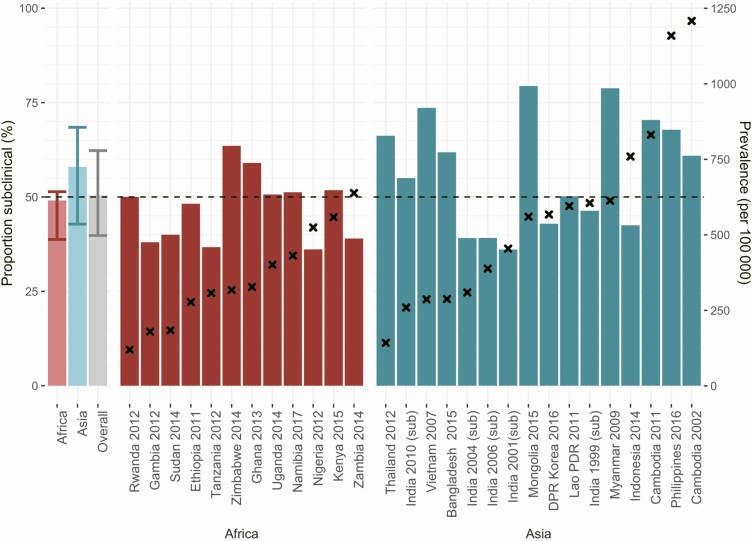
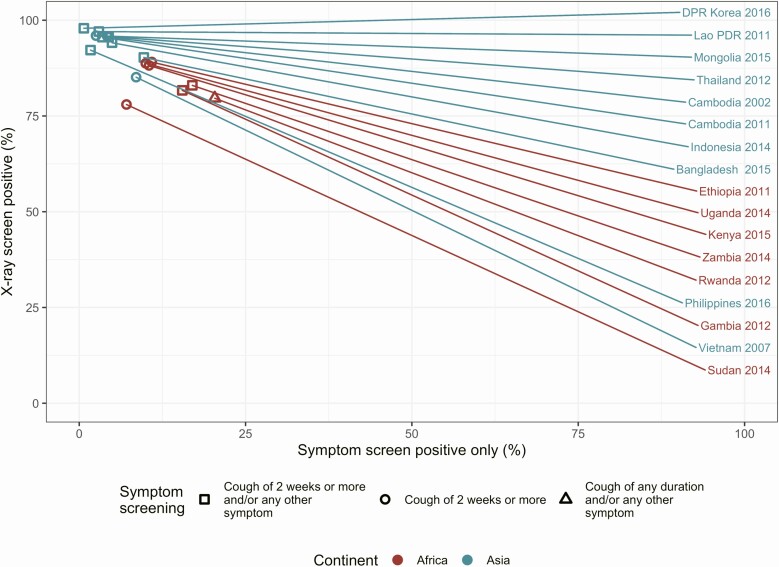
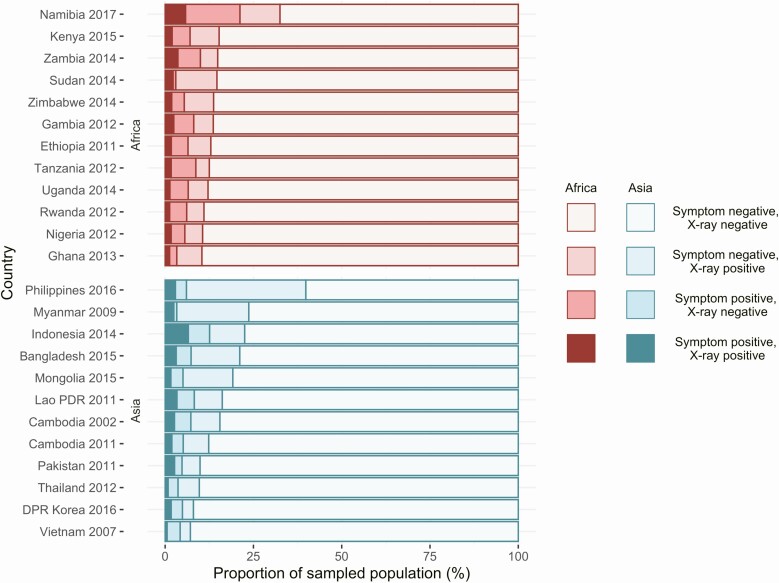
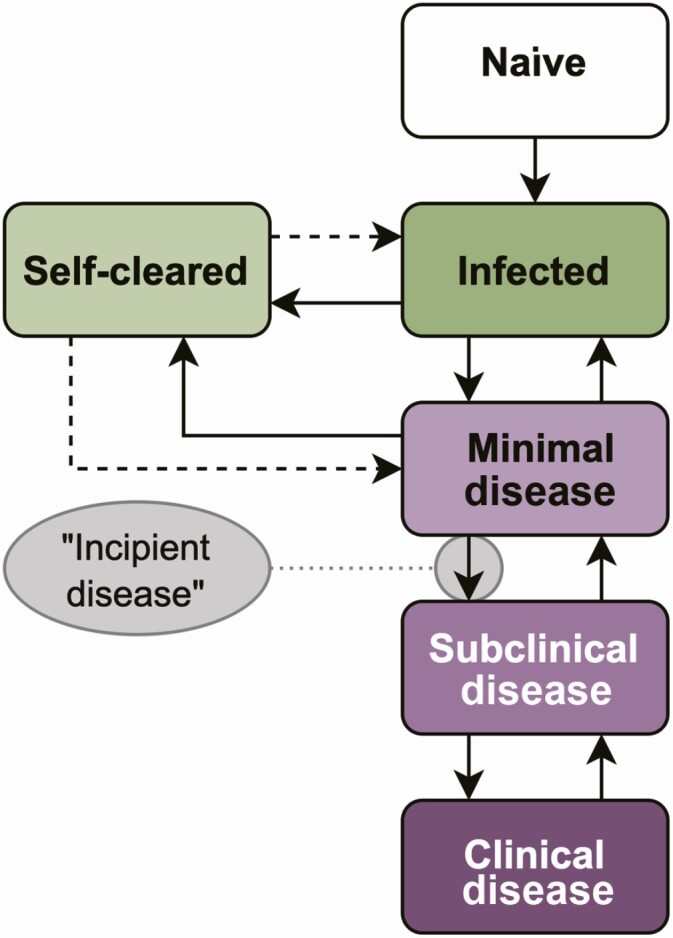
While it is known that a substantial proportion of individuals with tuberculosis disease (TB) present subclinically, usually defined as bacteriologically-confirmed but negative on symptom screening, considerable knowledge gaps remain. Our aim was to review data from TB prevalence population surveys and generate a consistent definition and framework for subclinical TB, enabling us to estimate the proportion of TB that is subclinical, explore associations with overall burden and program indicators, and evaluate the performance of screening strategies. We extracted data from all publicly available prevalence surveys conducted since 1990. Between 36.1% and 79.7% (median, 50.4%) of prevalent bacteriologically confirmed TB was subclinical. No association was found between prevalence of subclinical and all bacteriologically confirmed TB, patient diagnostic rate, or country-level HIV prevalence (P values, .32, .4, and .34, respectively). Chest Xray detected 89% (range, 73%-98%) of bacteriologically confirmed TB, highlighting the potential of optimizing current TB case-finding policies.
Keywords: TB prevalence surveys; TB screening; chest X-ray screening; subclinical TB; symptom screening.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- World Health Organization. Global tuberculosis report 2019. Available at: http://www.who.int/tb/publications/global_report/en/. Accessed 13 November 2019.
-
- World Health Organization. Systematic screening for active tuberculosis: principles and recommendations. Geneva, Switzerland: World Health Organization, 2013. - PubMed
-
- Esmail H, Dodd PJ, Houben RMGJ. Tuberculosis transmission during the subclinical period: could unrelated cough play a part? Lancet Respir Med 2018; 6:244–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
