

High levels of SARS-CoV-2-specific T cells with restricted functionality in severe courses of COVID-19
- PMID: 32937615
- PMCID: PMC7605520
- DOI: 10.1172/jci.insight.142167
High levels of SARS-CoV-2-specific T cells with restricted functionality in severe courses of COVID-19
Abstract
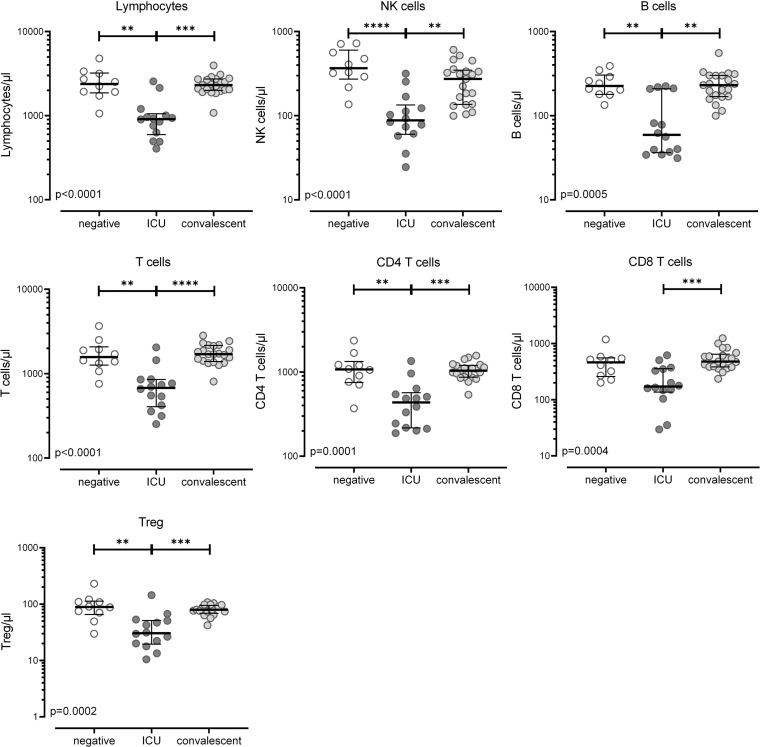
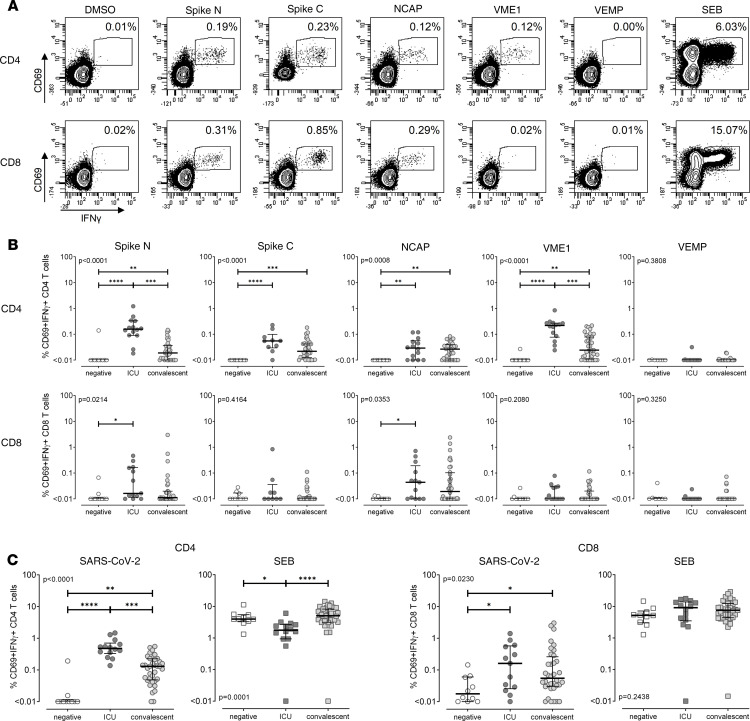
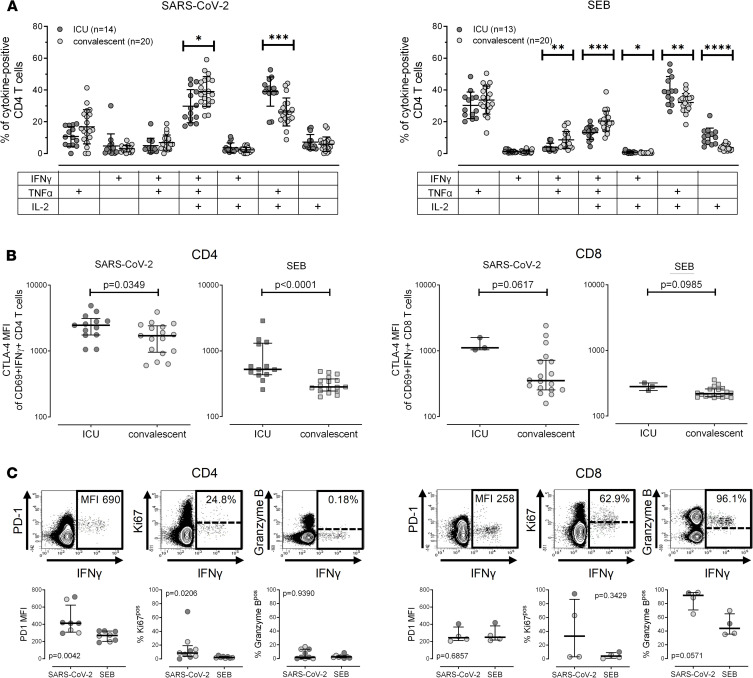
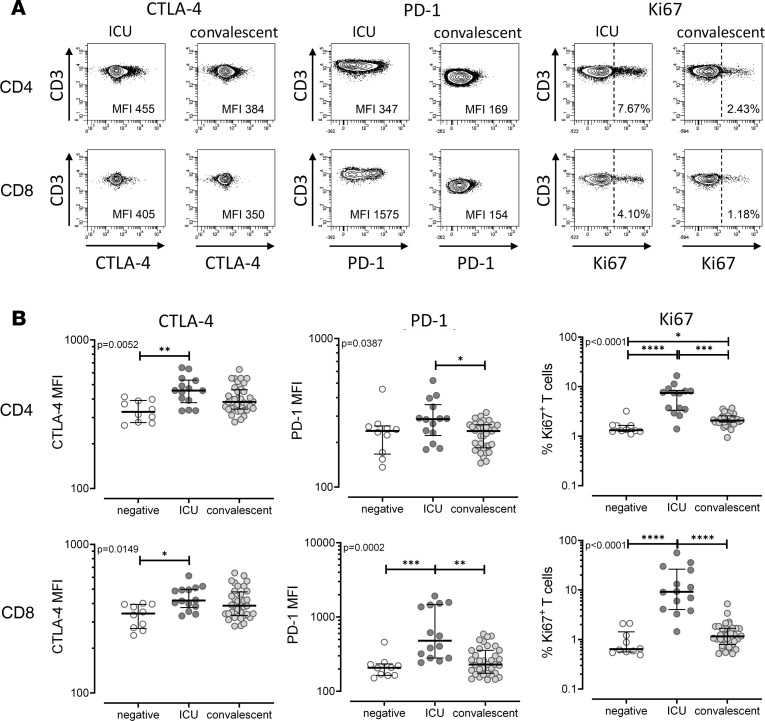
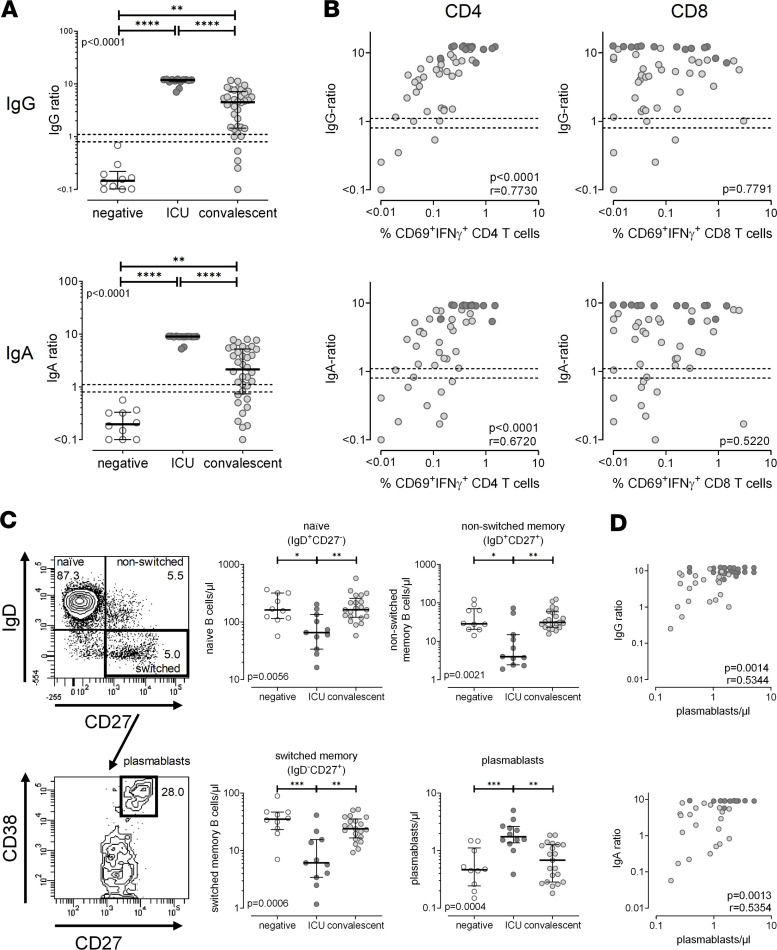
BACKGROUNDPatients infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) differ in the severity of disease. We hypothesized that characteristics of SARS-CoV-2-specific immunity correlate with disease severity.METHODSIn this study, SARS-CoV-2-specific T cells and antibodies were characterized in uninfected controls and patients with different coronavirus disease 2019 (COVID-19) disease severity. SARS-CoV-2-specific T cells were flow cytometrically quantified after stimulation with SARS-CoV-2 peptide pools and analyzed for expression of cytokines (IFN-γ, IL-2, and TNF-α) and markers for activation, proliferation, and functional anergy. SARS-CoV-2-specific IgG and IgA antibodies were quantified using ELISA. Moreover, global characteristics of lymphocyte subpopulations were compared between patient groups and uninfected controls.RESULTSDespite severe lymphopenia affecting all major lymphocyte subpopulations, patients with severe disease mounted significantly higher levels of SARS-CoV-2-specific T cells as compared with convalescent individuals. SARS-CoV-2-specific CD4+ T cells dominated over CD8+ T cells and closely correlated with the number of plasmablasts and SARS-CoV-2-specific IgA and IgG levels. Unlike in convalescent patients, SARS-CoV-2-specific T cells in patients with severe disease showed marked alterations in phenotypical and functional properties, which also extended to CD4+ and CD8+ T cells in general.CONCLUSIONGiven the strong induction of specific immunity to control viral replication in patients with severe disease, the functionally altered characteristics may result from the need for contraction of specific and general immunity to counteract excessive immunopathology in the lung.FUNDINGThe study was supported by institutional funds to MS and in part by grants of Saarland University, the State of Saarland, and the Rolf M. Schwiete Stiftung.
Keywords: COVID-19; Cellular immune response; Immunoglobulins; T cells.
Conflict of interest statement
Figures
Similar articles
-
Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients.EBioMedicine. 2020 May;55:102763. doi: 10.1016/j.ebiom.2020.102763. Epub 2020 Apr 18. EBioMedicine. 2020. PMID: 32361250 Free PMC article.
-
Long-term infection of SARS-CoV-2 changed the body's immune status.Clin Immunol. 2020 Sep;218:108524. doi: 10.1016/j.clim.2020.108524. Epub 2020 Jul 11. Clin Immunol. 2020. PMID: 32659373 Free PMC article.
-
The laboratory tests and host immunity of COVID-19 patients with different severity of illness.JCI Insight. 2020 May 21;5(10):e137799. doi: 10.1172/jci.insight.137799. JCI Insight. 2020. PMID: 32324595 Free PMC article.
-
Immune response to SARS-CoV-2 and mechanisms of immunopathological changes in COVID-19.Allergy. 2020 Jul;75(7):1564-1581. doi: 10.1111/all.14364. Allergy. 2020. PMID: 32396996 Free PMC article. Review.
-
The role of cytokine profile and lymphocyte subsets in the severity of coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis.Life Sci. 2020 Oct 1;258:118167. doi: 10.1016/j.lfs.2020.118167. Epub 2020 Jul 29. Life Sci. 2020. PMID: 32735885 Free PMC article.
Cited by
-
Decreased complement C3 levels are associated with poor prognosis in patients with COVID-19: A retrospective cohort study.Int Immunopharmacol. 2020 Dec;89(Pt A):107070. doi: 10.1016/j.intimp.2020.107070. Epub 2020 Oct 5. Int Immunopharmacol. 2020. PMID: 33039965 Free PMC article.
-
High-resolution analysis of individual spike peptide-specific CD4+ T-cell responses in vaccine recipients and COVID-19 patients.Clin Transl Immunology. 2022 Aug 9;11(8):e1410. doi: 10.1002/cti2.1410. eCollection 2022. Clin Transl Immunology. 2022. PMID: 35957961 Free PMC article.
-
PD-L1 Dysregulation in COVID-19 Patients.Front Immunol. 2021 Jun 7;12:695242. doi: 10.3389/fimmu.2021.695242. eCollection 2021. Front Immunol. 2021. PMID: 34163490 Free PMC article.
-
Increased B-cell activity with consumption of activated monocytes in severe COVID-19 patients.Eur J Immunol. 2021 Jun;51(6):1449-1460. doi: 10.1002/eji.202049163. Epub 2021 Apr 19. Eur J Immunol. 2021. PMID: 33788264 Free PMC article. Clinical Trial.
-
Exploring antibody repurposing for COVID-19: beyond presumed roles of therapeutic antibodies.Sci Rep. 2021 May 13;11(1):10220. doi: 10.1038/s41598-021-89621-6. Sci Rep. 2021. PMID: 33986382 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
