

Platelets Can Associate with SARS-Cov-2 RNA and Are Hyperactivated in COVID-19
- PMID: 32938299
- PMCID: PMC7641188
- DOI: 10.1161/CIRCRESAHA.120.317703
Platelets Can Associate with SARS-Cov-2 RNA and Are Hyperactivated in COVID-19
Abstract
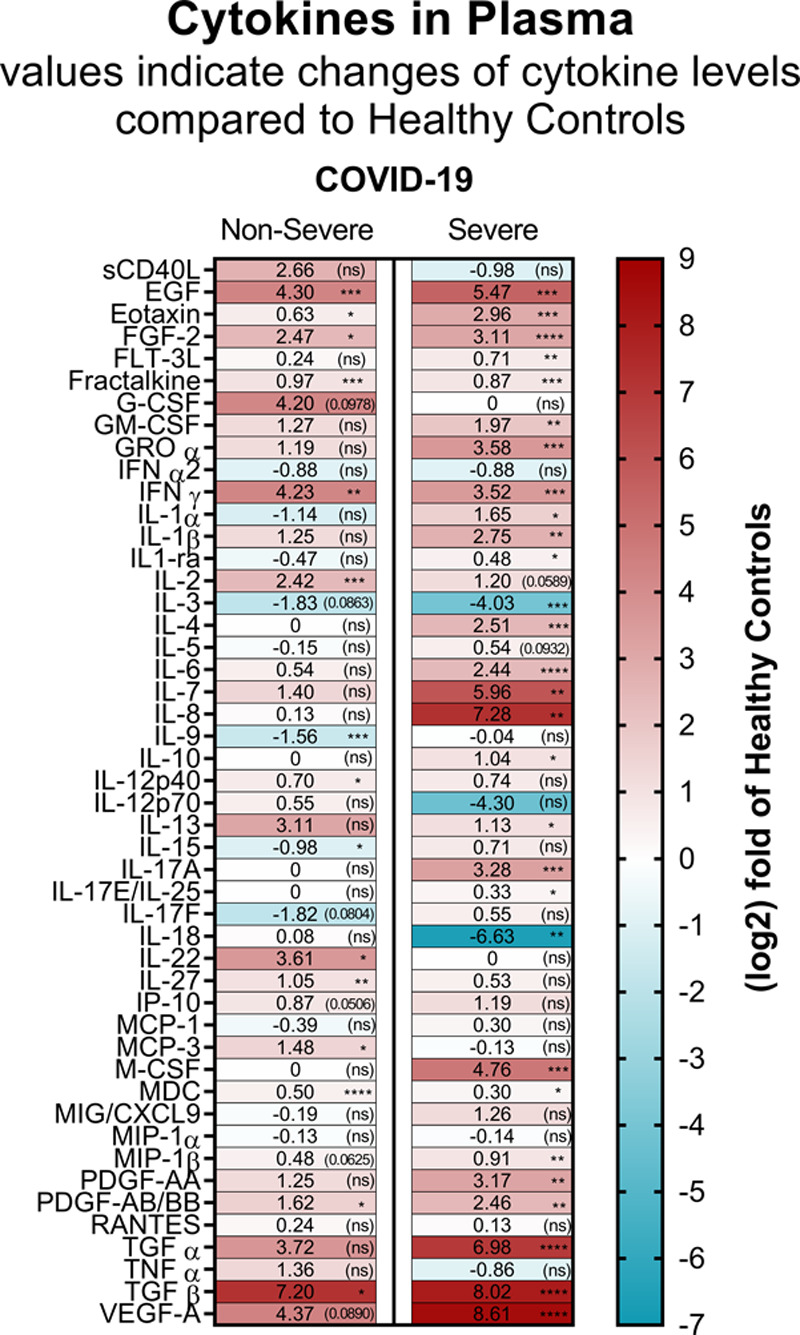
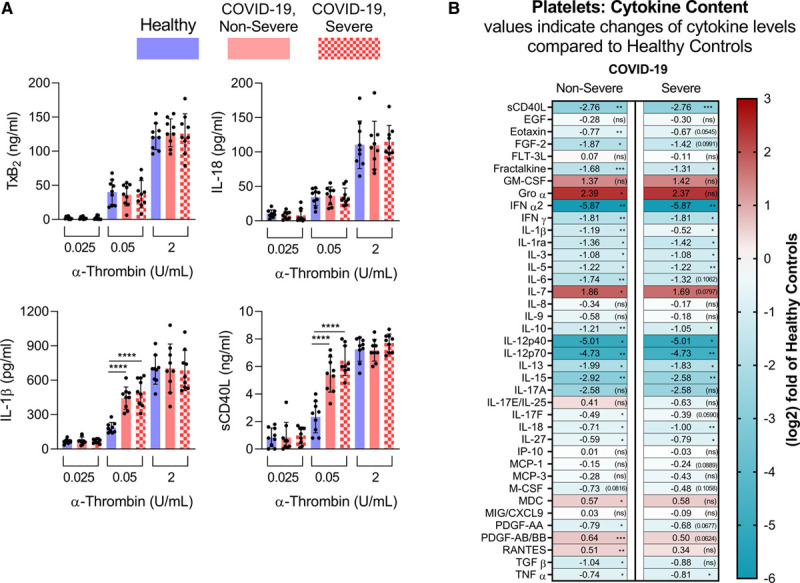
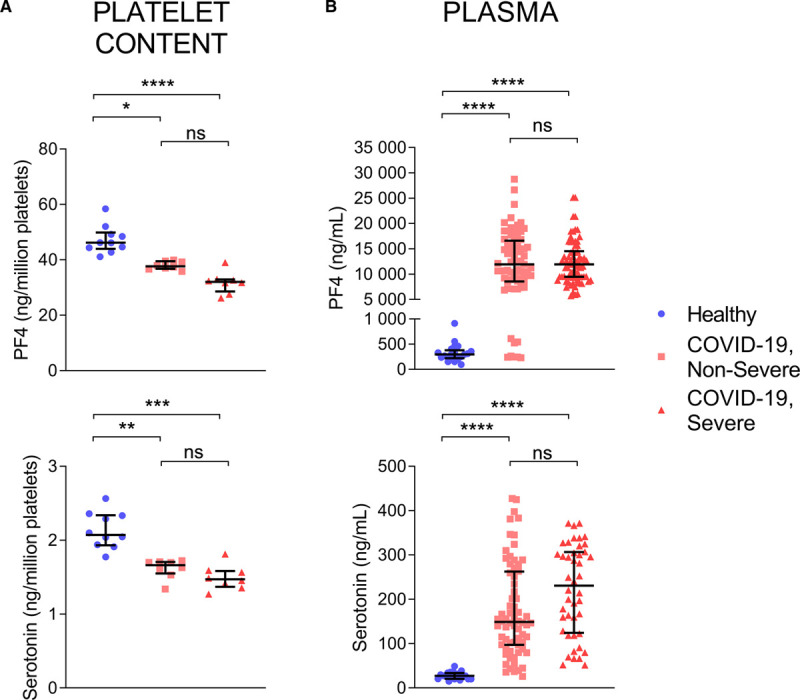
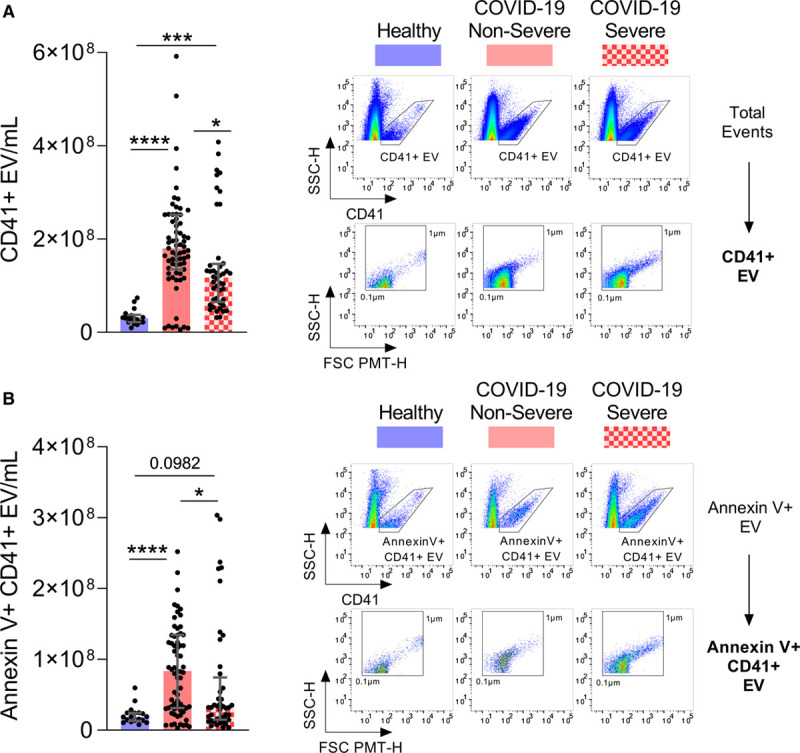
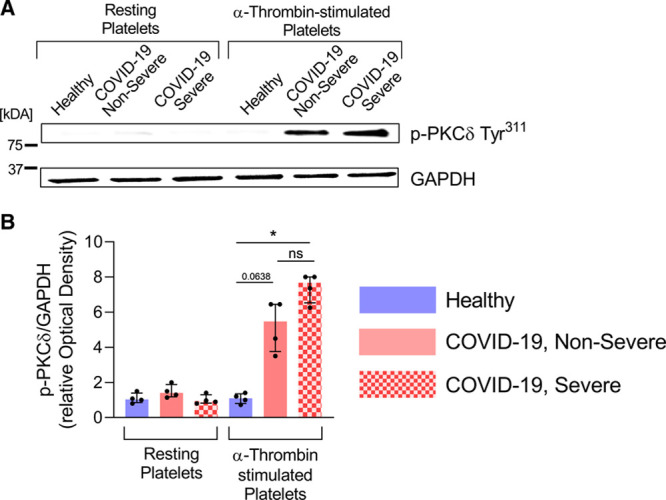
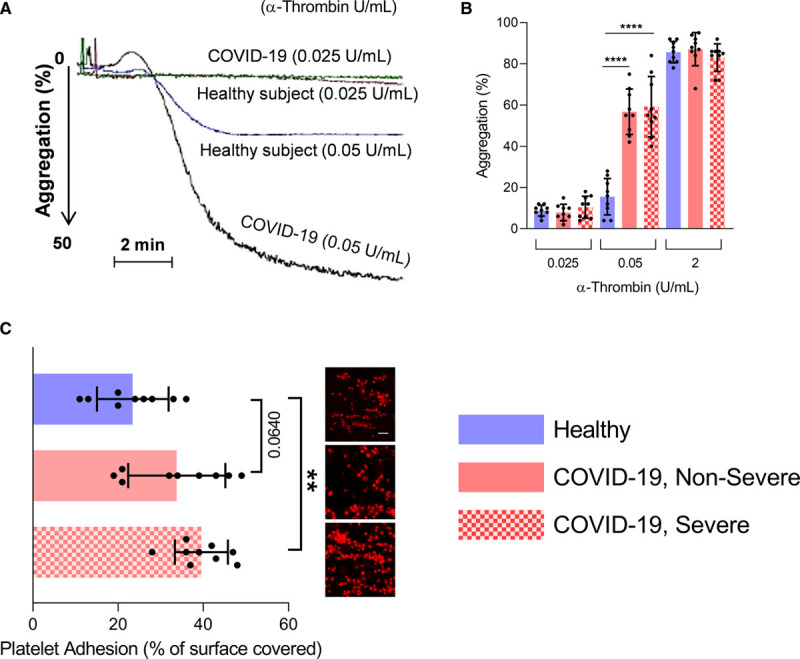
Rationale: In addition to the overwhelming lung inflammation that prevails in COVID-19, hypercoagulation and thrombosis contribute to the lethality of subjects infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Platelets are chiefly implicated in thrombosis. Moreover, they can interact with viruses and are an important source of inflammatory mediators. While a lower platelet count is associated with severity and mortality, little is known about platelet function during COVID-19. Objective: To evaluate the contribution of platelets to inflammation and thrombosis in COVID-19 patients. Methods and Results: Blood was collected from 115 consecutive COVID-19 patients presenting non-severe (n=71) and severe (n=44) respiratory symptoms. We document the presence of SARS-CoV-2 RNA associated with platelets of COVID-19 patients. Exhaustive assessment of cytokines in plasma and in platelets revealed the modulation of platelet-associated cytokine levels in both non-severe and severe COVID-19 patients, pointing to a direct contribution of platelets to the plasmatic cytokine load. Moreover, we demonstrate that platelets release their alpha- and dense-granule contents in both non-severe and severe forms of COVID-19. In comparison to concentrations measured in healthy volunteers, phosphatidylserine-exposing platelet extracellular vesicles were increased in non-severe, but not in severe cases of COVID-19. Levels of D-dimers, a marker of thrombosis, failed to correlate with any measured indicators of platelet activation. Functionally, platelets were hyperactivated in COVID-19 subjects presenting non-severe and severe symptoms, with aggregation occurring at suboptimal thrombin concentrations. Furthermore, platelets adhered more efficiently onto collagen-coated surfaces under flow conditions. Conclusions: Taken together, the data suggest that platelets are at the frontline of COVID-19 pathogenesis, as they release various sets of molecules through the different stages of the disease. Platelets may thus have the potential to contribute to the overwhelming thrombo-inflammation in COVID-19, and the inhibition of pathways related to platelet activation may improve the outcomes during COVID-19.
Keywords: SARS-CoV-2.
Conflict of interest statement
None.
Figures
Comment in
-
Platelets and COVID-19: Inflammation, Hyperactivation and Additional Questions.Circ Res. 2020 Nov 6;127(11):1419-1421. doi: 10.1161/CIRCRESAHA.120.318218. Epub 2020 Nov 5. Circ Res. 2020. PMID: 33151798 Free PMC article. No abstract available.
References
-
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2020https://covid19.who.int CdC-WhOpoM. Accessed September 14, 2020
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
