

Larger Nephron Size and Nephrosclerosis Predict Progressive CKD and Mortality after Radical Nephrectomy for Tumor and Independent of Kidney Function
- PMID: 32938650
- PMCID: PMC7608955
- DOI: 10.1681/ASN.2020040449
Larger Nephron Size and Nephrosclerosis Predict Progressive CKD and Mortality after Radical Nephrectomy for Tumor and Independent of Kidney Function
Abstract
Background: Nephron hypertrophy and nephrosclerosis may be important determinants of CKD and mortality. However, studies of outcomes associated with these microstructural features have been limited to small tissue specimens from patients selected for either good kidney health or known kidney disease.
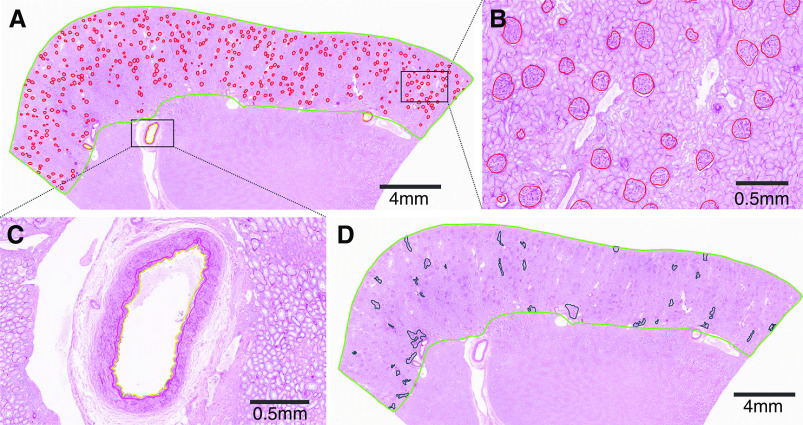
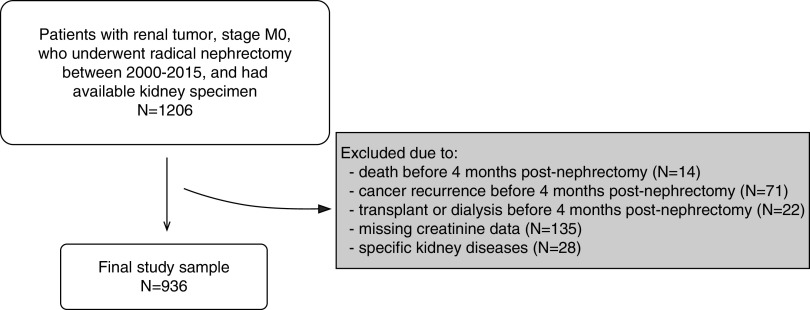
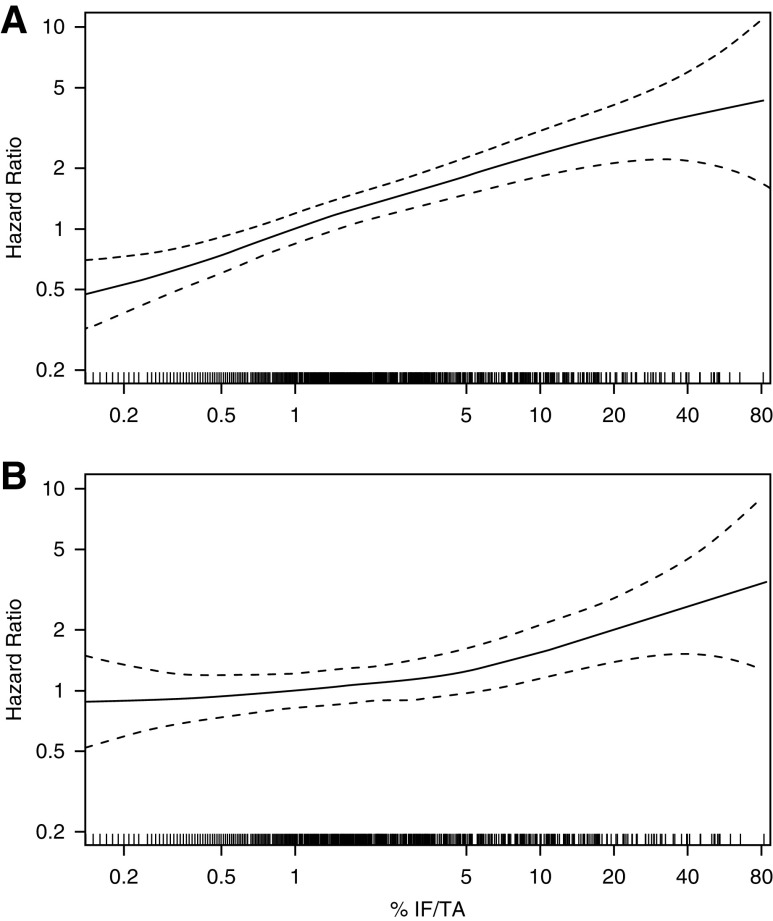
Methods: To determine whether microstructural features are predictive of progressive CKD and mortality outcomes, we studied patients who underwent a radical nephrectomy for a tumor. Large wedge sections of renal parenchyma distal to the tumor were stained and scanned into high-resolution images; we annotated the cortex and all glomeruli to calculate glomerular volume, cortex volume per glomerulus, and percentage of globally sclerotic glomeruli. Morphometric measurements also included percentages of artery luminal stenosis and interstitial fibrosis/tubular atrophy (IF/TA) of the cortex. At follow-up visits every 6-12 months, we determined which patients experienced progressive CKD (defined as dialysis, kidney transplantation, or a 40% decline from postnephrectomy eGFR). Cox models for these outcomes were adjusted for age, sex, body mass index, hypertension, diabetes, smoking, eGFR, and proteinuria.
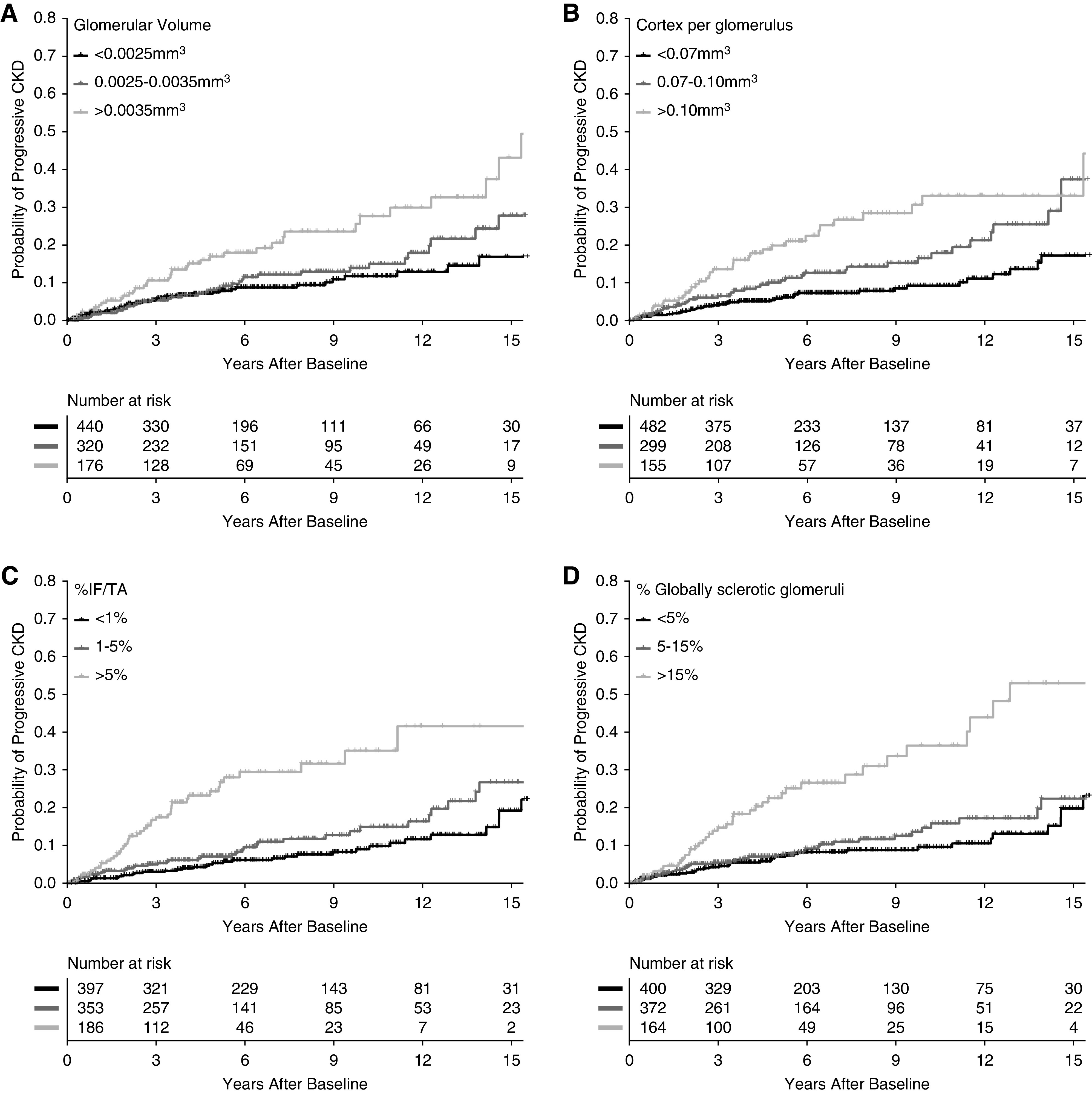
Results: Among 936 patients (mean age, 64 years; postnephrectomy baseline eGFR, 48 ml/min per 1.73 m2), 117 progressive CKD events, 183 noncancer deaths, and 116 cancer deaths occurred during a median follow-up of 6.4 years. Larger glomerular volume, larger cortex per glomerulus, and higher percentage of globally sclerotic glomeruli or IF/TA predicted progressive CKD. Higher percentage IF/TA also predicted noncancer mortality. Microstructural features did not predict cancer mortality or recurrence.
Conclusions: After a radical nephrectomy, larger nephrons and nephrosclerosis predicted progressive CKD, and IF/TA predicted noncancer mortality. Morphometric analysis of renal parenchyma can predict noncancer clinical events in patients long after their radical nephrectomy.
Keywords: Nephrectomy; glomerulosclerosis; glomerulus; interstitial fibrosis; kidney biopsy; mortality risk; nephron; progression of chronic renal failure.
Copyright © 2020 by the American Society of Nephrology.
Figures
Comment in
-
Can Total Nephron Number Predict Progressive CKD after Radical Nephrectomy?J Am Soc Nephrol. 2021 Feb;32(2):517. doi: 10.1681/ASN.2020111585. Epub 2020 Dec 17. J Am Soc Nephrol. 2021. PMID: 34103379 Free PMC article. No abstract available.
-
Authors' Reply.J Am Soc Nephrol. 2021 Feb;32(2):517-518. doi: 10.1681/ASN.2020111615. Epub 2020 Dec 17. J Am Soc Nephrol. 2021. PMID: 34103392 Free PMC article. No abstract available.
Similar articles
-
A Higher Foci Density of Interstitial Fibrosis and Tubular Atrophy Predicts Progressive CKD after a Radical Nephrectomy for Tumor.J Am Soc Nephrol. 2021 Oct;32(10):2623-2633. doi: 10.1681/ASN.2021020267. Epub 2021 Jun 18. J Am Soc Nephrol. 2021. PMID: 34531177 Free PMC article.
-
Tubular and Glomerular Size by Cortex Depth as Predictor of Progressive CKD after Radical Nephrectomy for Tumor.J Am Soc Nephrol. 2023 Sep 1;34(9):1535-1545. doi: 10.1681/ASN.0000000000000180. Epub 2023 Jul 11. J Am Soc Nephrol. 2023. PMID: 37430426 Free PMC article.
-
Age-Based Versus Young-Adult Thresholds for Nephrosclerosis on Kidney Biopsy and Prognostic Implications for CKD.J Am Soc Nephrol. 2023 Aug 1;34(8):1421-1432. doi: 10.1681/ASN.0000000000000171. Epub 2023 May 31. J Am Soc Nephrol. 2023. PMID: 37254246 Free PMC article.
-
Aging-Related Kidney Diseases.Contrib Nephrol. 2021;199:266-273. doi: 10.1159/000517708. Epub 2021 Aug 3. Contrib Nephrol. 2021. PMID: 34343996 Review.
-
Tubular atrophy in the pathogenesis of chronic kidney disease progression.Pediatr Nephrol. 2016 May;31(5):693-706. doi: 10.1007/s00467-015-3169-4. Epub 2015 Jul 25. Pediatr Nephrol. 2016. PMID: 26208584 Free PMC article. Review.
Cited by
-
Glomerular Hypertrophy and Initial Dip in Estimated Glomerular Filtration Rate Following Dapagliflozin Administration.Kidney Int Rep. 2024 Apr 27;9(7):2282-2285. doi: 10.1016/j.ekir.2024.04.046. eCollection 2024 Jul. Kidney Int Rep. 2024. PMID: 39081734 Free PMC article. No abstract available.
-
Glomerular hyperfiltration and hypertrophy: an evaluation of maximum values in pathological indicators to discriminate "diseased" from "normal".Front Med (Lausanne). 2023 Jul 13;10:1179834. doi: 10.3389/fmed.2023.1179834. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37521339 Free PMC article. Review.
-
Authors' Reply.J Am Soc Nephrol. 2021 Feb;32(2):517-518. doi: 10.1681/ASN.2020111615. Epub 2020 Dec 17. J Am Soc Nephrol. 2021. PMID: 34103392 Free PMC article. No abstract available.
-
Effect of Dataset Size and Medical Image Modality on Convolutional Neural Network Model Performance for Automated Segmentation: A CT and MR Renal Tumor Imaging Study.J Digit Imaging. 2023 Aug;36(4):1770-1781. doi: 10.1007/s10278-023-00804-1. Epub 2023 Mar 17. J Digit Imaging. 2023. PMID: 36932251 Free PMC article.
-
AI in the Loop: functionalizing fold performance disagreement to monitor automated medical image segmentation workflows.Front Radiol. 2023 Sep 15;3:1223294. doi: 10.3389/fradi.2023.1223294. eCollection 2023. Front Radiol. 2023. PMID: 37780641 Free PMC article.
References
-
- Gautam G, Lifshitz D, Shikanov S, Moore JM, Eggener SE, Shalhav AL, et al. : Histopathological predictors of renal function decrease after laparoscopic radical nephrectomy. J Urol 184: 1872–1876, 2010. - PubMed
-
- Salvatore SP, Cha EK, Rosoff JS, Seshan SV: Nonneoplastic renal cortical scarring at tumor nephrectomy predicts decline in kidney function. Arch Pathol Lab Med 137: 531–540, 2013. - PubMed
-
- Brandina R, Moreira Leite KR, Gregório EP, Fernandes KBP, Srougi M: Histologic abnormalities in non-neoplastic renal parenchyma and the risk of chronic kidney disease following radical nephrectomy. Urology 100: 158–162, 2017. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
