

Maxillary protraction using customized mini-plates for anchorage in an adolescent girl with skeletal Class III malocclusion
- PMID: 32938827
- PMCID: PMC7500574
- DOI: 10.4041/kjod.2020.50.5.346
Maxillary protraction using customized mini-plates for anchorage in an adolescent girl with skeletal Class III malocclusion
Abstract
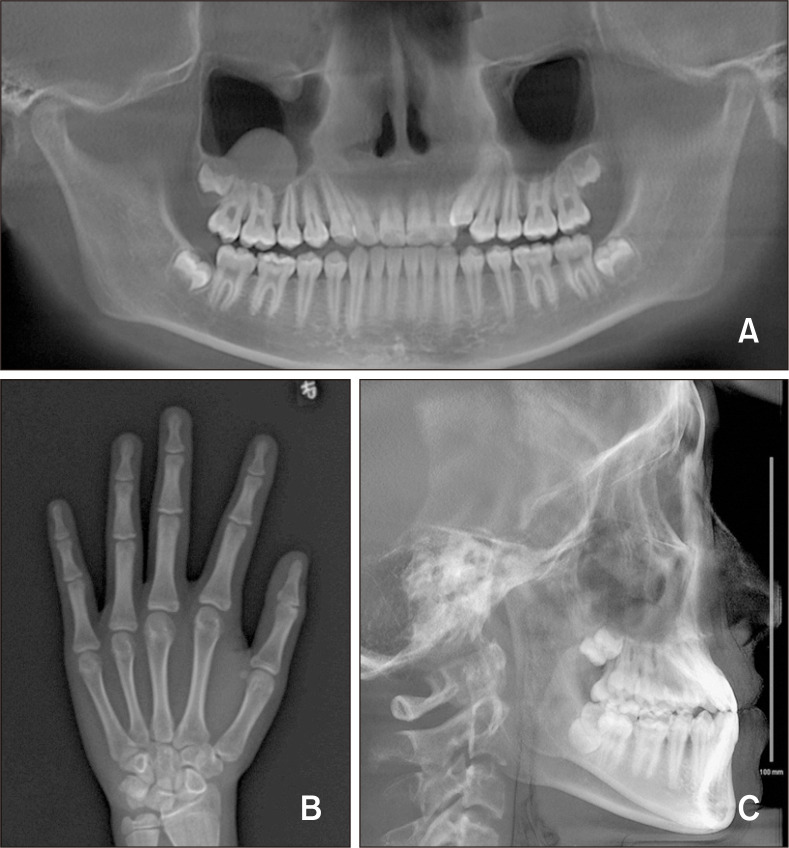
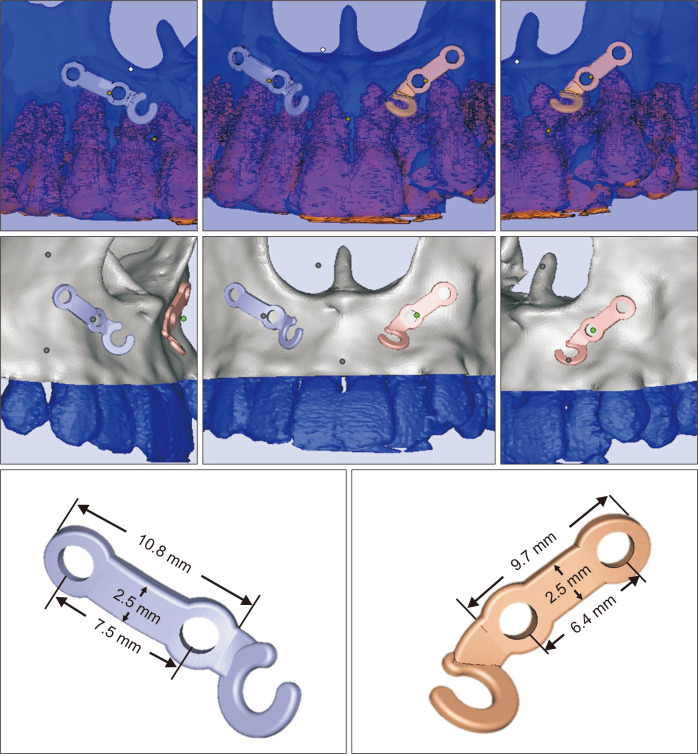
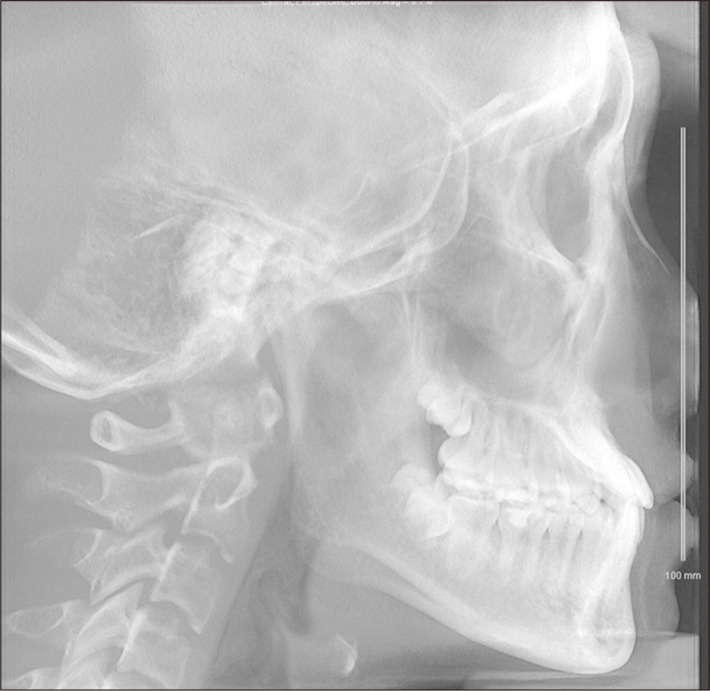
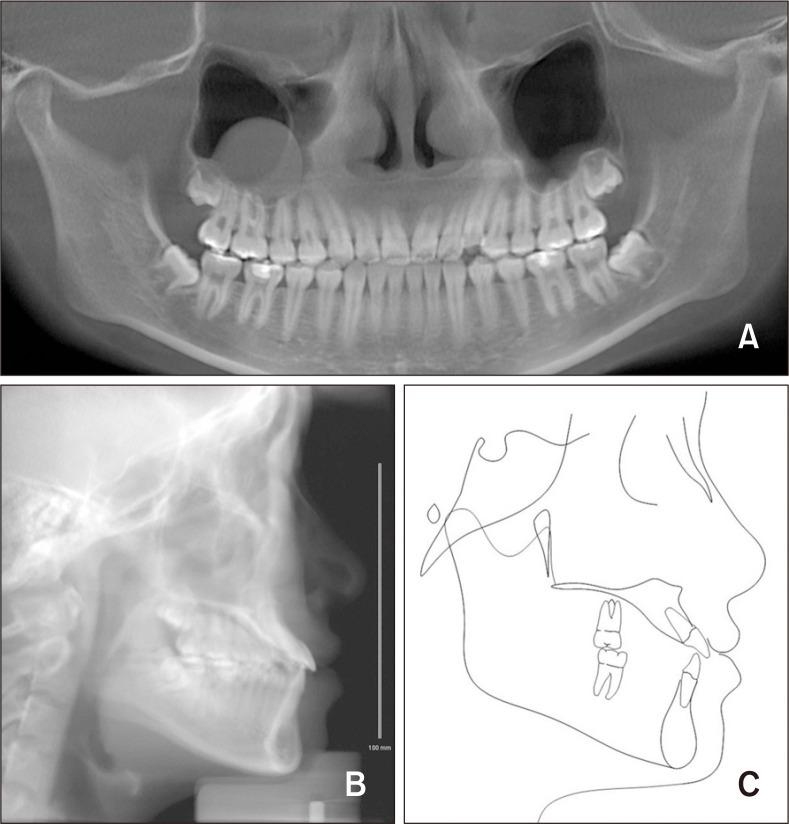
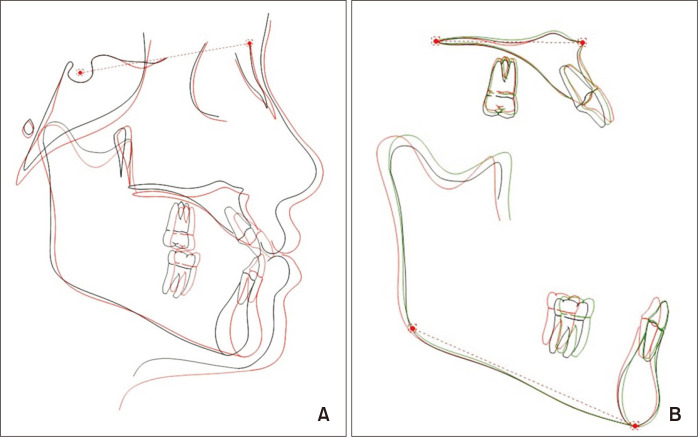
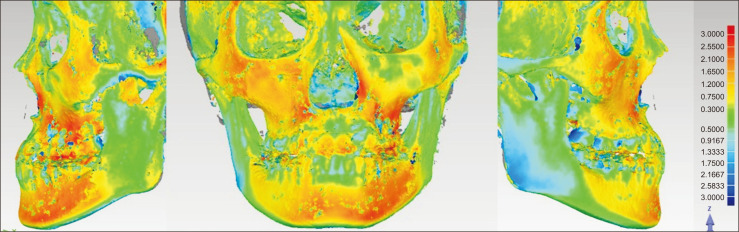
The treatment of skeletal Class III malocclusion in adolescents is challenging. Maxillary protraction, particularly that using bone anchorage, has been proven to be an effective method for the stimulation of maxillary growth. However, the conventional procedure, which involves the surgical implantation of mini-plates, is traumatic and associated with a high risk. Three-dimensional (3D) digital technology offers the possibility of individualized treatment. Customized miniplates can be designed according to the shape of the maxillary surface and the positions of the roots on cone-beam computed tomography scans; this reduces both the surgical risk and patient trauma. Here we report a case involving a 12-year-old adolescent girl with skeletal Class III malocclusion and midface deficiency that was treated in two phases. In phase 1, rapid maxillary expansion and protraction were performed using 3D-printed mini-plates for anchorage. The mini-plates exhibited better adaptation to the bone contour, and titanium screw implantation was safer because of the customized design. The orthopedic force applied to each mini-plate was approximately 400-500 g, and the plates remained stable during the maxillary protraction process, which exhibited efficacious orthopedic effects and significantly improved the facial profile and esthetics. In phase 2, fixed appliances were used for alignment and leveling of the maxillary and mandibular dentitions. The complete two-phase treatment lasted for 24 months. After 48 months of retention, the treatment outcomes remained stable.
Keywords: Customized mini-plates; Face mask; Implant design; Threedimensional printing.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures




References
-
- Allwright WC, Bundred WH. A survey of handicapping dentofacial anomalies among Chinese in Hong Kong. Int Dent J. 1964;14:505–19.
Publication types
LinkOut - more resources
Full Text Sources