

Safety and Immunogenicity of Heterologous and Homologous 2-Dose Regimens of Adenovirus Serotype 26- and Modified Vaccinia Ankara-Vectored Ebola Vaccines: A Randomized, Controlled Phase 1 Study
- PMID: 32939546
- PMCID: PMC9441209
- DOI: 10.1093/infdis/jiaa586
Safety and Immunogenicity of Heterologous and Homologous 2-Dose Regimens of Adenovirus Serotype 26- and Modified Vaccinia Ankara-Vectored Ebola Vaccines: A Randomized, Controlled Phase 1 Study
Abstract
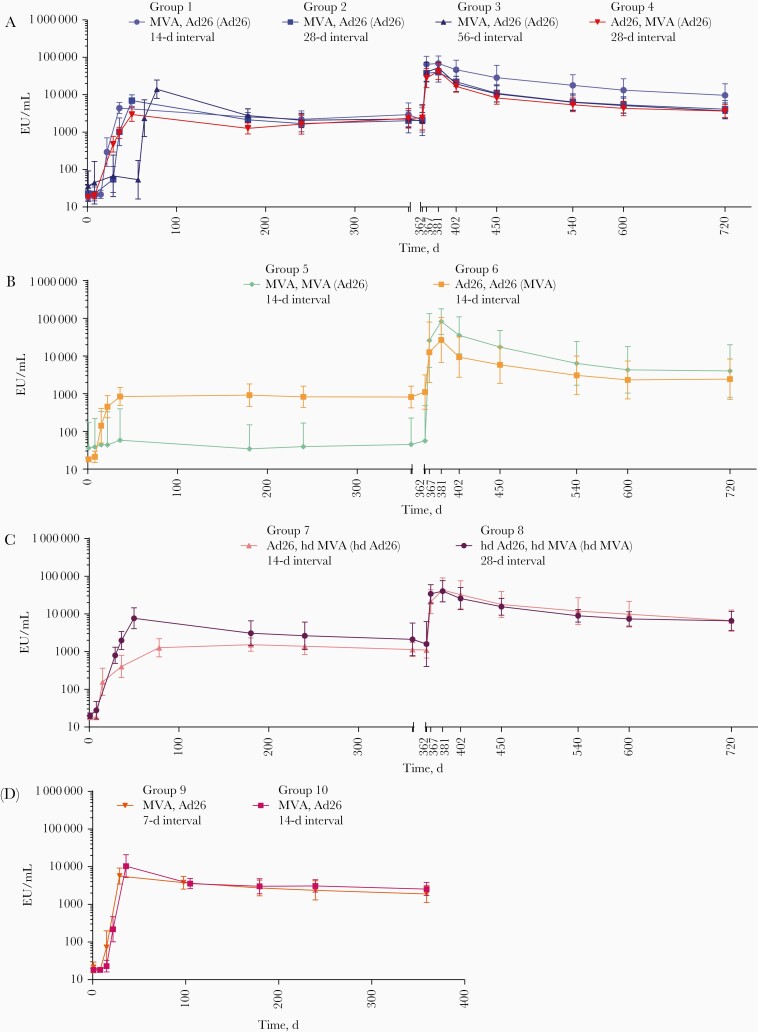
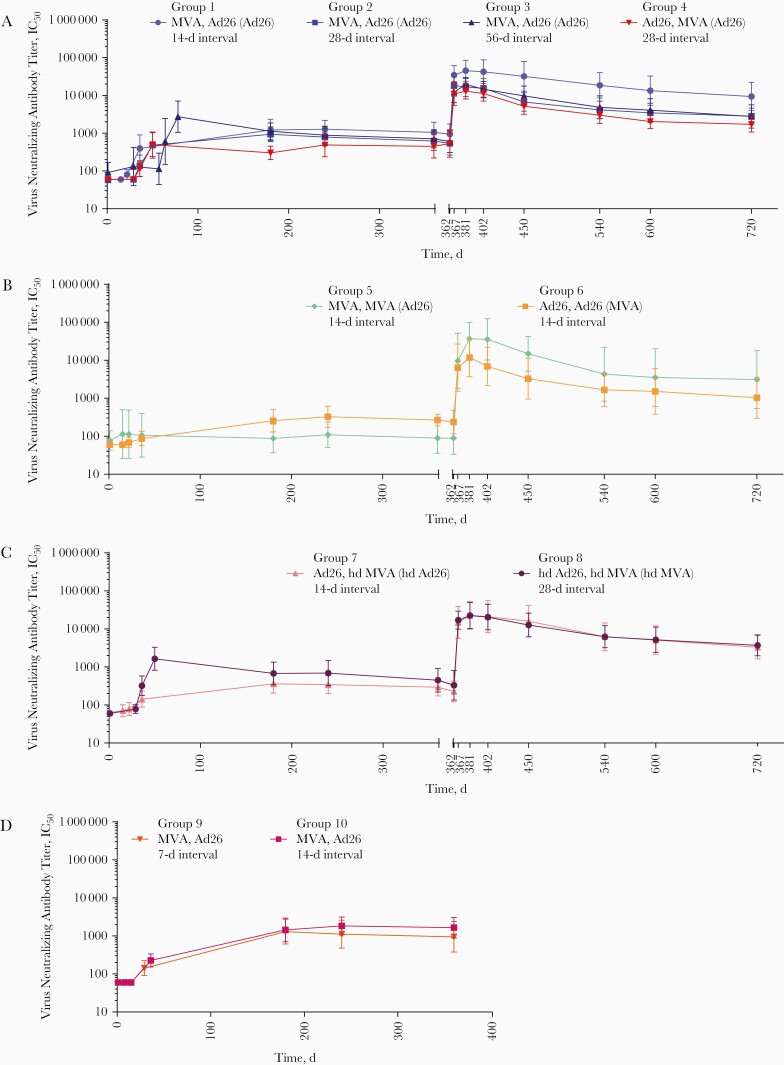
Background: This phase 1 placebo-controlled study assessed the safety and immunogenicity of 2-dose regimens of Ad26.ZEBOV (adenovirus serotype 26 [Ad26]) and MVA-BN-Filo (modified vaccinia Ankara [MVA]) vaccines with booster vaccination at day 360.
Methods: Healthy US adults (N = 164) randomized into 10 groups received saline placebo or standard or high doses of Ad26 or MVA in 2-dose regimens at 7-, 14-, 28-, or 56-day intervals; 8 groups received booster Ad26 or MVA vaccinations on day 360. Participants reported solicited and unsolicited reactogenicity; we measured immunoglobulin G binding, neutralizing antibodies and cellular immune responses to Ebola virus glycoprotein.
Results: All regimens were well tolerated with no serious vaccine-related adverse events. Heterologous (Ad26,MVA [dose 1, dose 2] or MVA,Ad26) and homologous (Ad26,Ad26) regimens induced humoral and cellular immune responses 21 days after dose 2; responses were higher after heterologous regimens. Booster vaccination elicited anamnestic responses in all participants.
Conclusions: Both heterologous and homologous Ad26,MVA Ebola vaccine regimens are well tolerated in healthy adults, regardless of interval or dose level. Heterologous 2-dose Ad26,MVA regimens containing an Ebola virus insert induce strong, durable humoral and cellular immune responses. Immunological memory was rapidly recalled by booster vaccination, suggesting that Ad26 booster doses could be considered for individuals at risk of Ebola infection, who previously received the 2-dose regimen.
Keywords: 2-dose; Ad26.ZEBOV; Ebola vaccine; MVA-BN-Filo; heterologous; homologous; immunogenicity; safety.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures

References
-
- Malvy D, McElroy AK, de Clerck H, Günther S, van Griensven J. Ebola virus disease. Lancet 2019; 393:936–48. - PubMed
-
- Centers for Disease Control and Prevention. Ebola virus disease distribution map: cases of Ebola virus disease in Africa since 1976. https://www.cdc.gov/vhf/ebola/history/distribution-map.html/. Accessed 10 August 2020.
-
- Burki T. Ebola in the Democratic Republic of the Congo: 1 year on. Lancet Infect Dis 2019; 19:813–4. - PubMed
-
- World Health Organization . Ebola in the Democratic Republic of the Congo—health emergency update. https://www.who.int/emergencies/diseases/ebola/drc-2019. Accessed 10 August 2020.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
