

Architectural Alterations in Oral Epithelial Dysplasia are Similar in Unifocal and Proliferative Leukoplakia
- PMID: 32939744
- PMCID: PMC8134567
- DOI: 10.1007/s12105-020-01216-1
Architectural Alterations in Oral Epithelial Dysplasia are Similar in Unifocal and Proliferative Leukoplakia
Abstract
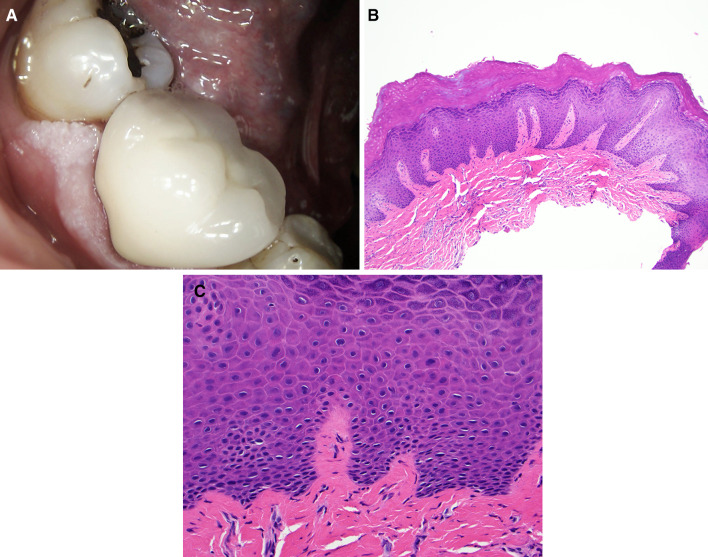
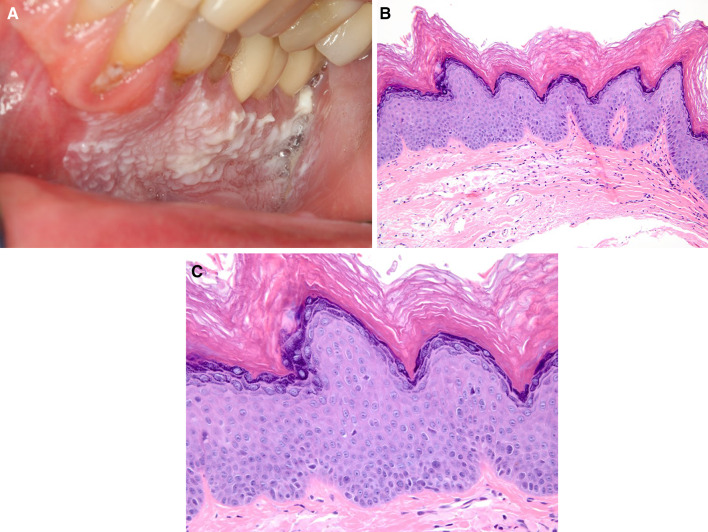
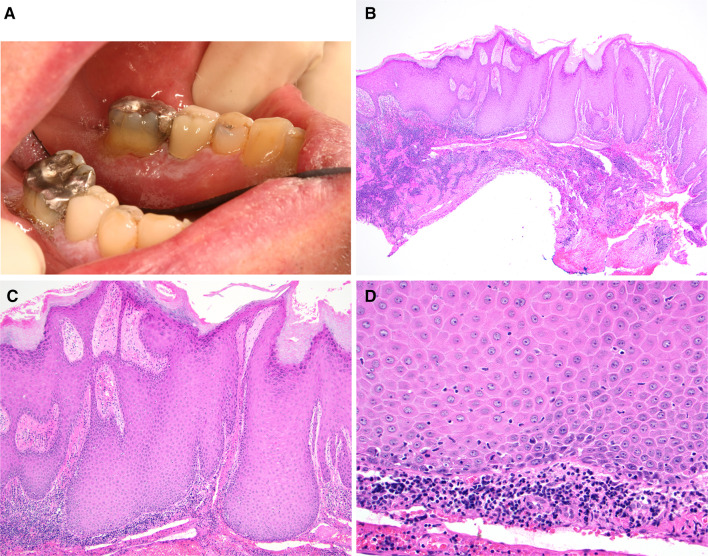
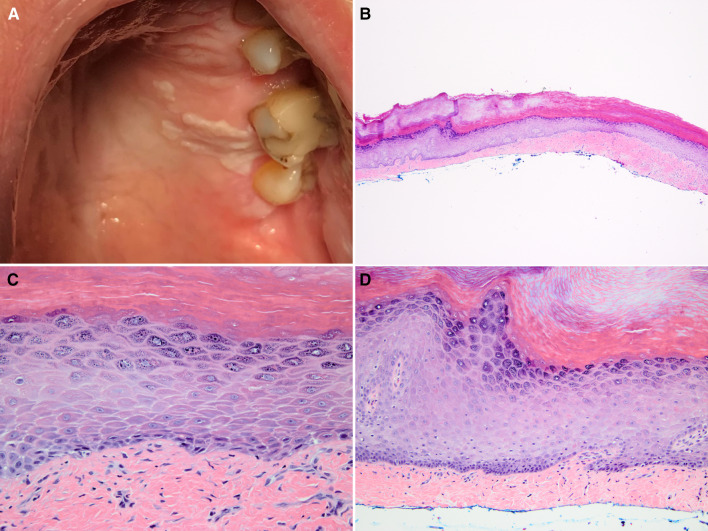
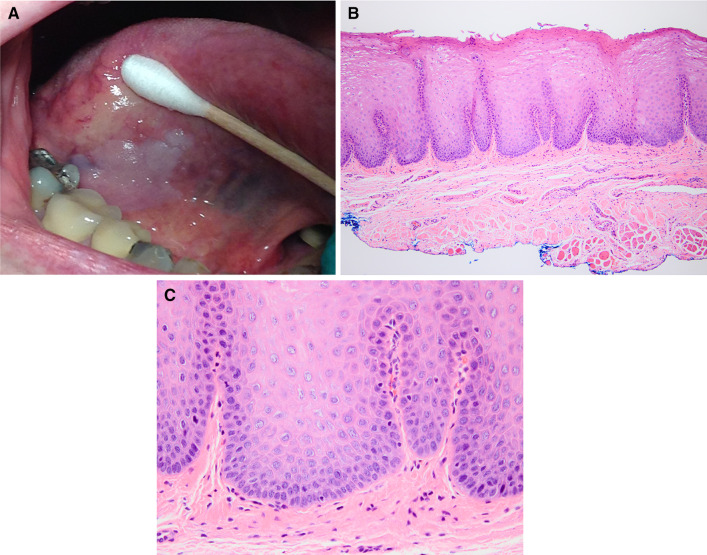
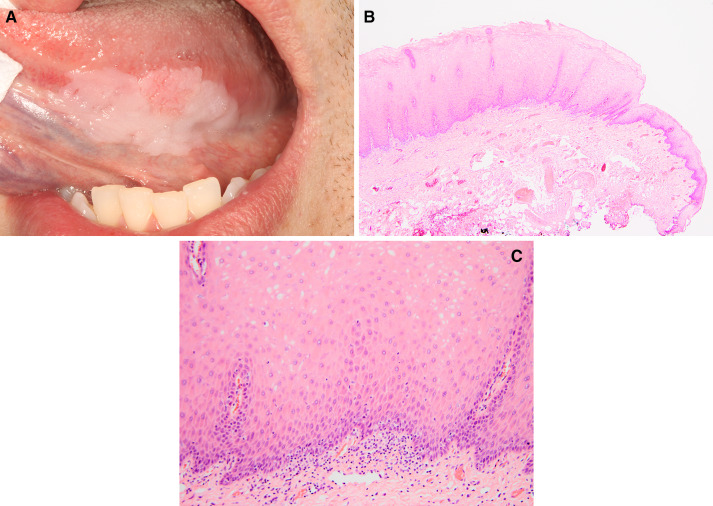
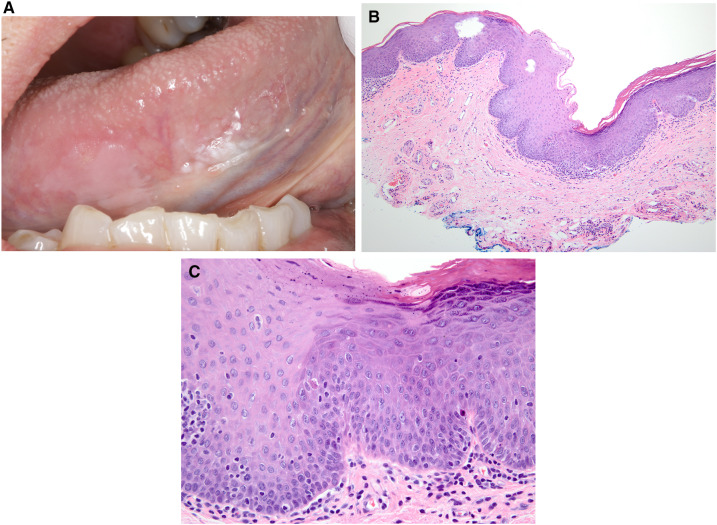
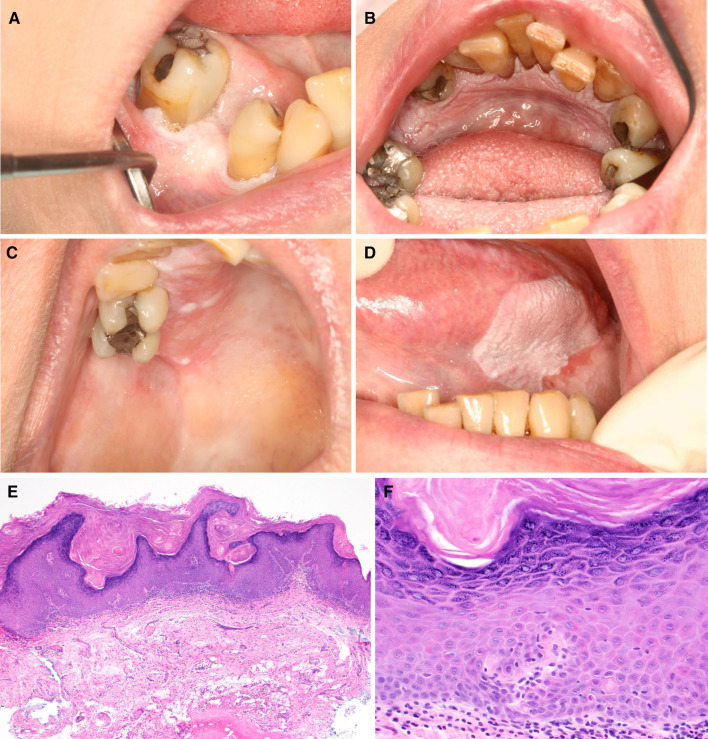
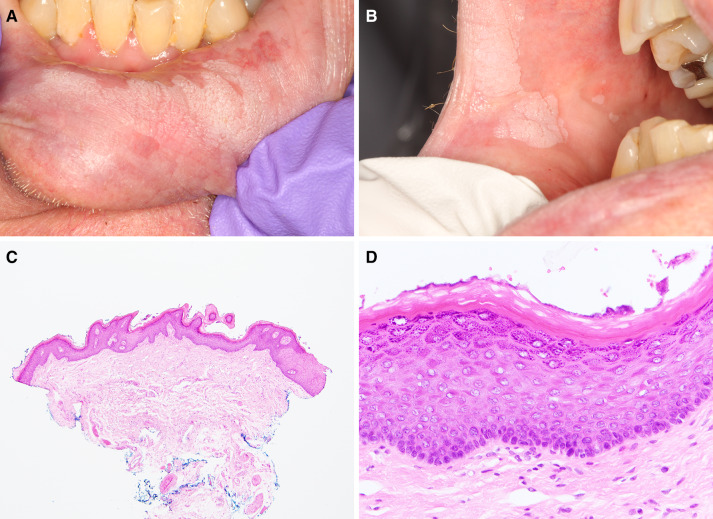
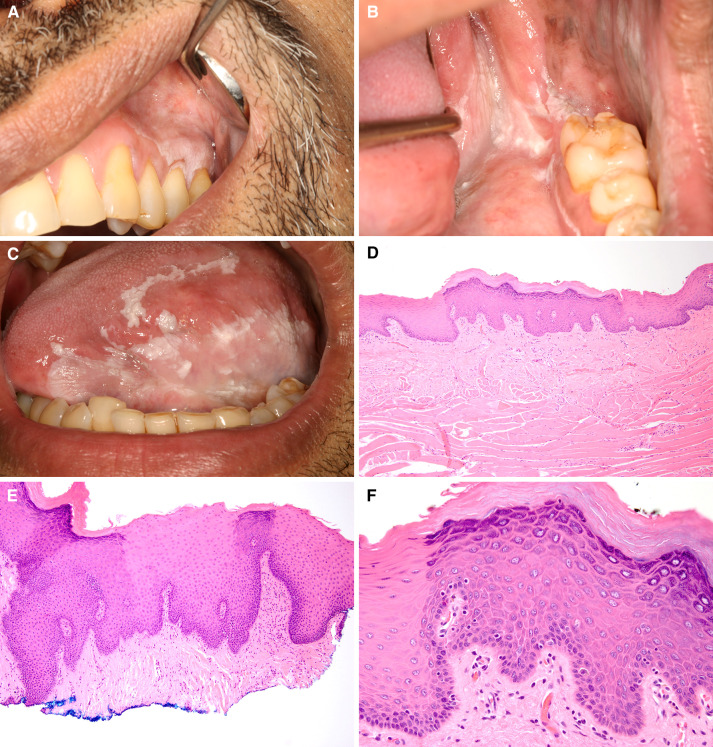
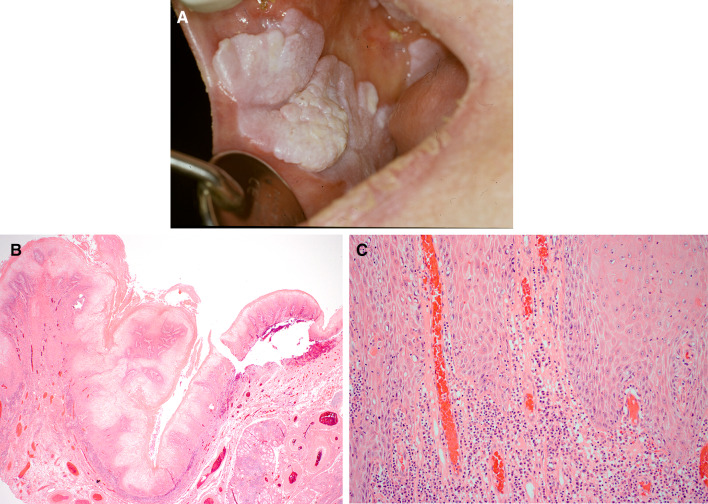
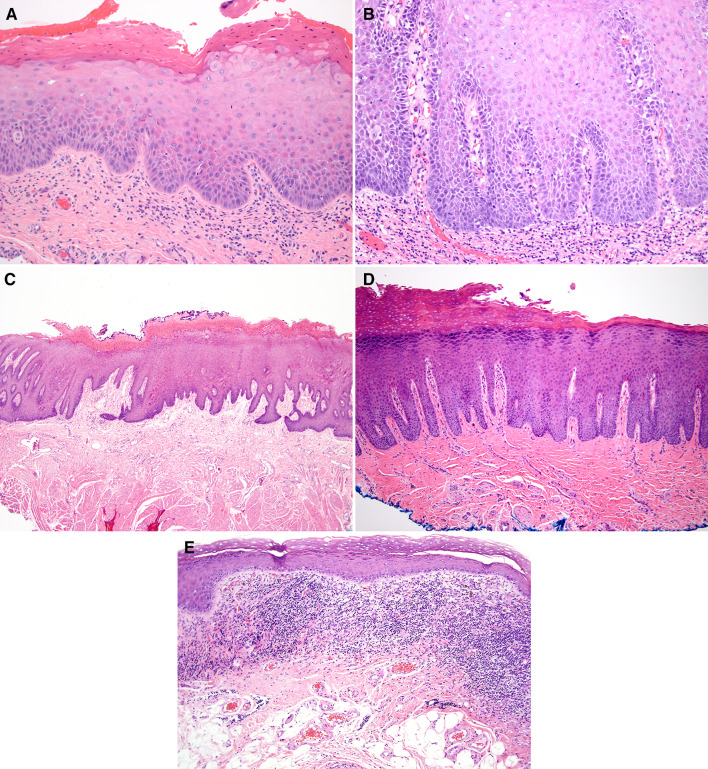
The current WHO histopathologic criteria for oral epithelial dysplasia (ED) are based on architectural and cytologic alterations, and do not address other histopathologic features of ED. Here we propose new diagnostic criteria including architectural, organizational, and cytologic features for oral ED. Cases of unifocal leukoplakia (UL) and proliferative leukoplakia (PL) with clinical photographs and follow-up information were identified. Only cases that showed minimal cytologic atypia or mild ED were used to demonstrate critical architectural changes as defined in this study. Eight biopsies from eight UL patients and 34 biopsies from four PL patients were included. The biopsies showed (a) corrugated, verrucous or papillary architecture, (b) hyperkeratosis with epithelial atrophy, (c) bulky squamous epithelial proliferation, and (d) demarcated hyperkeratosis and "skip" segments. The architectural alterations defined here are as important as the currently used criteria for the diagnosis of ED. Clinicopathologic correlation when diagnosing oral ED is also of the utmost importance in accurate diagnosis.
Keywords: Architectural alteration; Leukoplakia; Malignant transformation; Oral epithelial dysplasia; Proliferative verrucous leukoplakia.
Conflict of interest statement
No conflict of interest to disclose.
Figures

References
-
- Warnakulasuriya S, Johnson NW, van der Waal I. Nomenclature and classification of potentially malignant disorders of the oral mucosa. J Oral Pathol Med. 2007;36(10):575–580. - PubMed
-
- Reibel J, Gale N, Hille J, et al. Oral potentially malignant disorders and oral epithelial dysplasia. WHO Classif Head Neck Tumours. 2017;9:112.
-
- Woo SB, Grammer RL, Lerman MA. Keratosis of unknown significance and leukoplakia: a preliminary study. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014;118(6):713–724. - PubMed
-
- Napier SS, Speight PM. Natural history of potentially malignant oral lesions and conditions: an overview of the literature. J Oral Pathol Med. 2008;37(1):1–10. - PubMed
-
- Kumar A, Cascarini L, McCaul JA, et al. How should we manage oral leukoplakia? Br J Oral Maxillofacial Surg. 2013;51(5):377–383. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
