

Risk Prediction Models for Post-Operative Mortality in Patients With Cirrhosis
- PMID: 32939786
- PMCID: PMC7902392
- DOI: 10.1002/hep.31558
Risk Prediction Models for Post-Operative Mortality in Patients With Cirrhosis
Abstract
Background and aims: Patients with cirrhosis are at increased risk of postoperative mortality. Currently available tools to predict postoperative risk are suboptimally calibrated and do not account for surgery type. Our objective was to use population-level data to derive and internally validate cirrhosis surgical risk models.
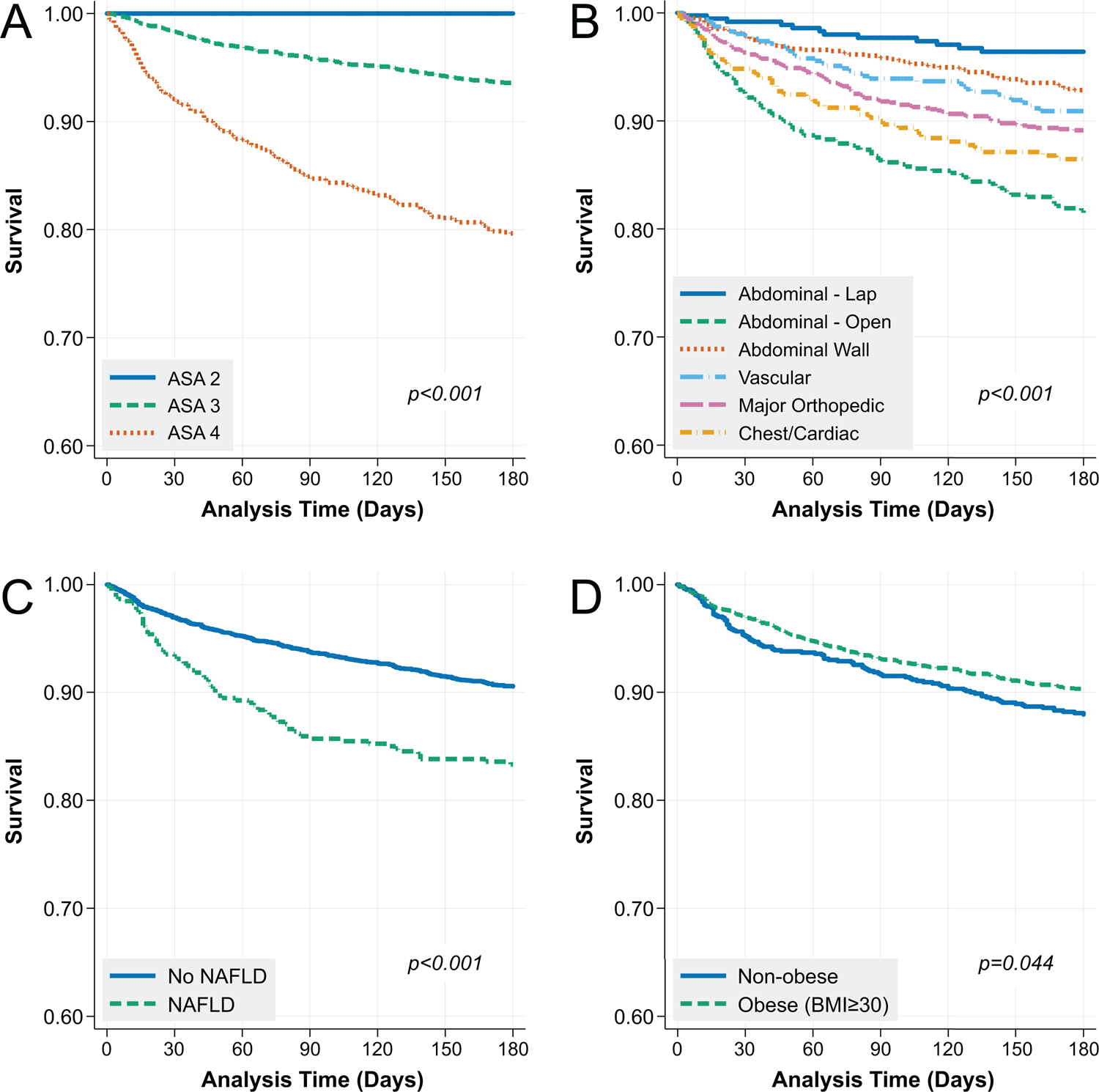
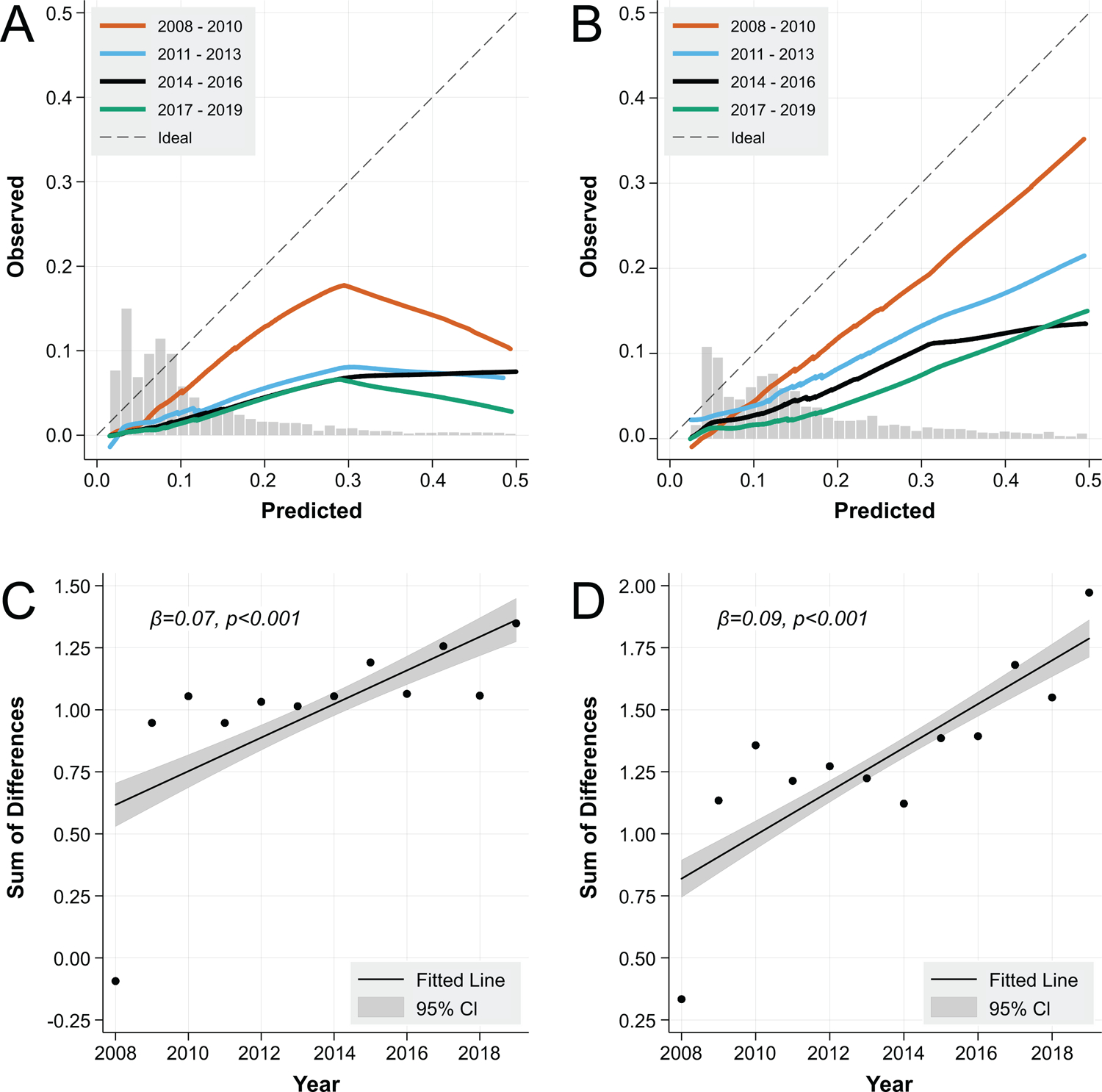
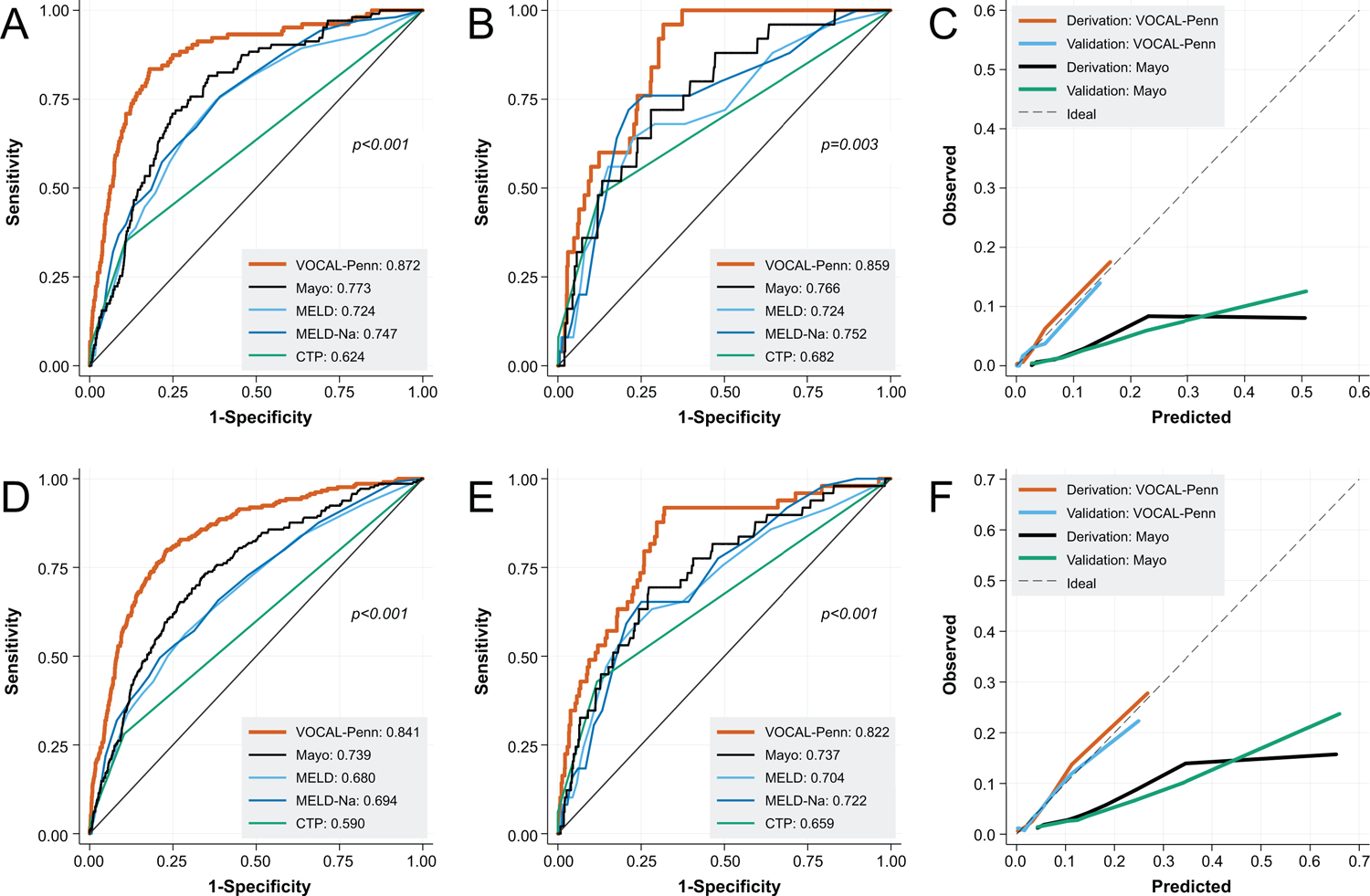
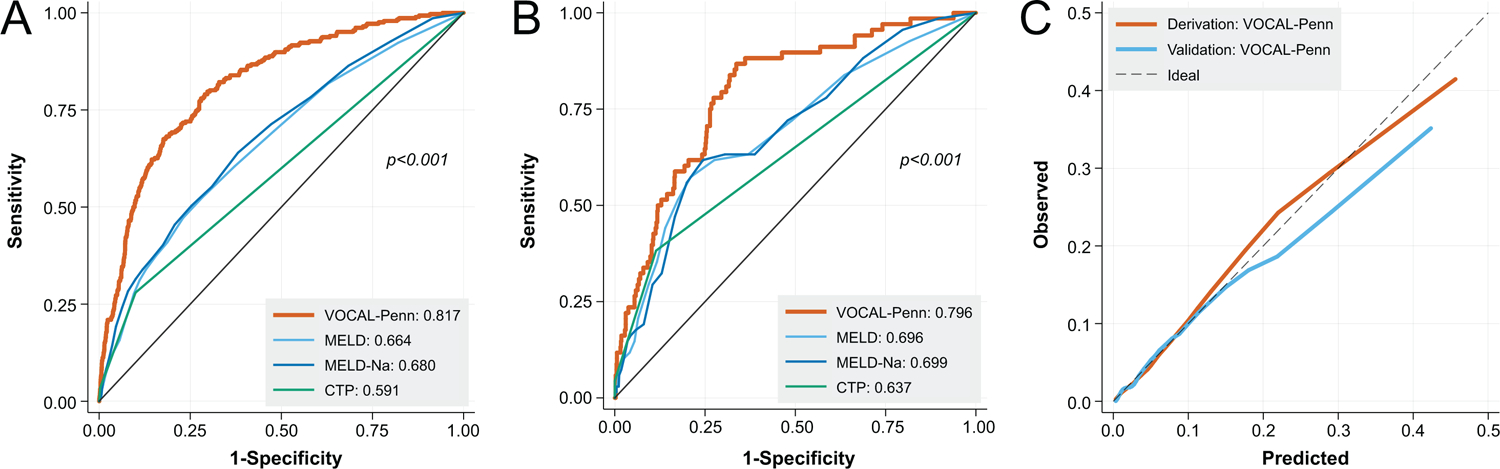
Approach and results: We conducted a retrospective cohort study using data from the Veterans Outcomes and Costs Associated with Liver Disease (VOCAL) cohort, which contains granular data on patients with cirrhosis from 128 U.S. medical centers, merged with the Veterans Affairs Surgical Quality Improvement Program (VASQIP) to identify surgical procedures. We categorized surgeries as abdominal wall, vascular, abdominal, cardiac, chest, or orthopedic and used multivariable logistic regression to model 30-, 90-, and 180-day postoperative mortality (VOCAL-Penn models). We compared model discrimination and calibration of VOCAL-Penn to the Mayo Risk Score (MRS), Model for End-Stage Liver Disease (MELD), Model for End-Stage Liver Disease-Sodium MELD-Na, and Child-Turcotte-Pugh (CTP) scores. We identified 4,712 surgical procedures in 3,785 patients with cirrhosis. The VOCAL-Penn models were derived and internally validated with excellent discrimination (30-day postoperative mortality C-statistic = 0.859; 95% confidence interval [CI], 0.809-0.909). Predictors included age, preoperative albumin, platelet count, bilirubin, surgery category, emergency indication, fatty liver disease, American Society of Anesthesiologists classification, and obesity. Model performance was superior to MELD, MELD-Na, CTP, and MRS at all time points (e.g., 30-day postoperative mortality C-statistic for MRS = 0.766; 95% CI, 0.676-0.855) in terms of discrimination and calibration.
Conclusions: The VOCAL-Penn models substantially improve postoperative mortality predictions in patients with cirrhosis. These models may be applied in practice to improve preoperative risk stratification and optimize patient selection for surgical procedures (www.vocalpennscore.com).
© 2020 by the American Association for the Study of Liver Diseases.
Conflict of interest statement
Figures
Comment in
-
Letter to the Editor: Evaluating Liver Function in Patients With Cirrhosis.Hepatology. 2021 Sep;74(3):1708. doi: 10.1002/hep.31626. Epub 2021 Aug 30. Hepatology. 2021. PMID: 33184905 No abstract available.
-
Selection of Patients With Cirrhosis For Surgery: As Much An Art As Science.Hepatology. 2021 Jan;73(1):7-9. doi: 10.1002/hep.31643. Hepatology. 2021. PMID: 33220099 No abstract available.
References
-
- Friedman LS. The risk of surgery in patients with liver disease. Hepatology 1999;29:1617–1623. - PubMed
-
- Goel NJ, Agarwal P, Mallela AN, et al. Liver disease is an independent predictor of poor 30-day outcomes following surgery for degenerative disease of the cervical spine. The Spine Journal 2019;19:448–460. - PubMed
-
- Johnson KM, Newman KL, Green PK, et al. Incidence and Risk Factors of Postoperative Mortality and Morbidity After Elective Versus Emergent Abdominal Surgery in a National Sample of 8193 Patients With Cirrhosis. Annals of surgery 2019. - PubMed
-
- Parikh ND, Marrero WJ, Wang J, et al. Projected increase in obesity and non-alcoholic-steatohepatitis–related liver transplantation waitlist additions in the United States. Hepatology 2019;70:487–495. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
