

Risk and predictors of dyssynchrony cardiomyopathy in left bundle branch block with preserved left ventricular ejection fraction
- PMID: 32940385
- PMCID: PMC7724243
- DOI: 10.1002/clc.23467
Risk and predictors of dyssynchrony cardiomyopathy in left bundle branch block with preserved left ventricular ejection fraction
Abstract
Background: Left bundle branch block (LBBB) and left ventricular (LV) dyssynchrony likely contribute to progressive systolic dysfunction. The evaluation of newly recognized LBBB includes screening for structural heart abnormalities and coronary artery disease (CAD). In patients whose LV ejection fraction (EF) is preserved during initial testing, the incidence of subsequent cardiomyopathy is not firmly established.
Hypothesis: The risk of developing LV systolic dysfunction among LBBB patients with preserved LVEF is high enough to warrant serial imaging.
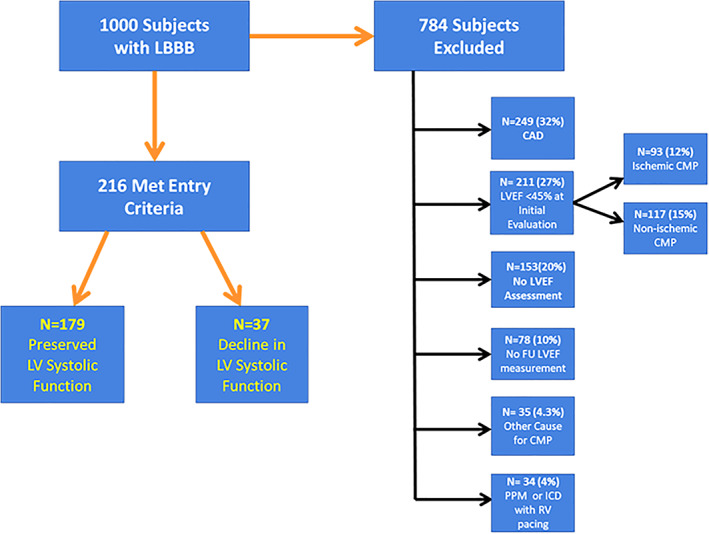
Methods: We screened records of 1000 consecutive patients with LBBB from our ECG database and identified subjects with an initially preserved LVEF (≥45%) without clinically relevant CAD or other cause for cardiomyopathy. Baseline imaging, clinical data, and follow-up imaging were recorded to determine the risk of subsequent LV systolic dysfunction (LVEF ≤40%).
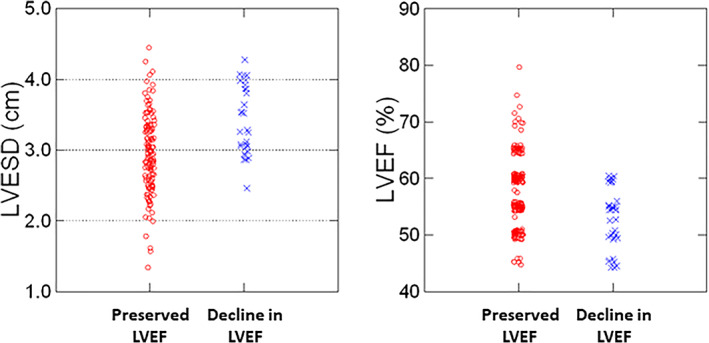
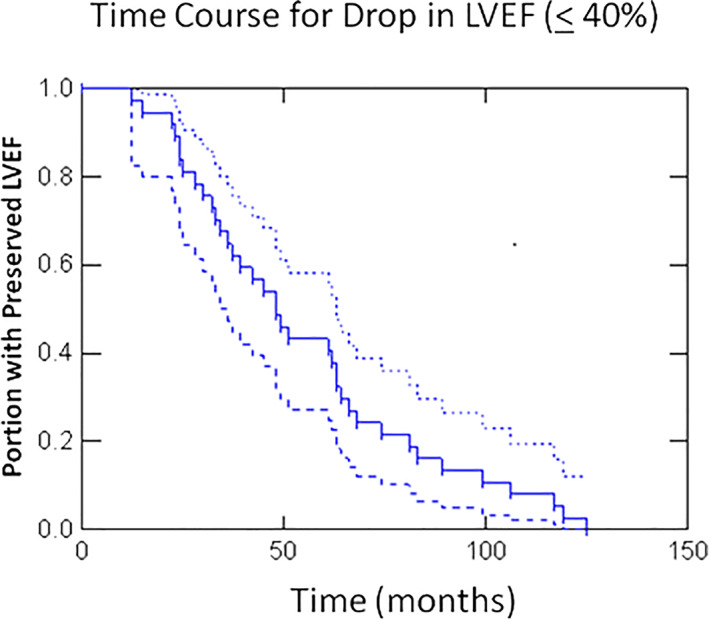
Results: (Data are mean + SD) 784 subjects were excluded, the majority for CAD or depressed LVEF upon initial imaging. Of the remaining 216, 37 (17%) developed a decline in LVEF(≤40%) over a mean follow-up of 55 ± 31 months; 94% of these patients had a baseline LVEF≤60% and LV end systolic diameter (ESD) ≥ 2.9 cm indicating that these measures may be useful to define which patients warrant longitudinal follow-up. The negative predictive value of a LVEF>60% and LVESD <2.9 cm was 98%.
Conclusions: Seventeen percent of patients with LBBB and initial preserved LVEF develop dyssynchrony cardiomyopathy. We believe the risk of developing dyssynchrony cardiomyopathy is high enough to warrant serial assessment of LV systolic function in this high-risk population.
Keywords: cardiomyopathy; dyssynchrony; heart failure; left bundle branch block.
© 2020 The Authors. Clinical Cardiology published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no potential conflict of interests.
Figures
Similar articles
-
Ventricular dyssynchrony of idiopathic versus pacing-induced left bundle branch block and its prognostic effect in patients with preserved left ventricular systolic function.Am J Cardiol. 2012 Feb 15;109(4):556-62. doi: 10.1016/j.amjcard.2011.09.048. Epub 2011 Nov 29. Am J Cardiol. 2012. PMID: 22133751
-
Outcomes with T-wave discordance of left bundle branch block and preserved or mildly reduced ejection fraction.ESC Heart Fail. 2024 Aug;11(4):2148-2158. doi: 10.1002/ehf2.14764. Epub 2024 Apr 12. ESC Heart Fail. 2024. PMID: 38607371 Free PMC article.
-
Prevalence and progression of LV dysfunction and dyssynchrony in patients with new-onset LBBB post TAVR.Cardiovasc Revasc Med. 2024 Nov;68:23-29. doi: 10.1016/j.carrev.2024.04.011. Epub 2024 Apr 5. Cardiovasc Revasc Med. 2024. PMID: 38604832
-
Mechanism of harm from left bundle branch block.Trends Cardiovasc Med. 2019 Aug;29(6):335-342. doi: 10.1016/j.tcm.2018.10.012. Epub 2018 Oct 25. Trends Cardiovasc Med. 2019. PMID: 30401603 Review.
-
Left bundle branch block-induced left ventricular remodeling and its potential for reverse remodeling.J Interv Card Electrophysiol. 2018 Aug;52(3):343-352. doi: 10.1007/s10840-018-0407-2. Epub 2018 Jul 17. J Interv Card Electrophysiol. 2018. PMID: 30019271 Review.
Cited by
-
2023 HRS/APHRS/LAHRS guideline on cardiac physiologic pacing for the avoidance and mitigation of heart failure.J Arrhythm. 2023 Aug 2;39(5):681-756. doi: 10.1002/joa3.12872. eCollection 2023 Oct. J Arrhythm. 2023. PMID: 37799799 Free PMC article.
-
Left bundle branch block cardiomyopathy (LBBB-CMP): from the not-so-benign finding of idiopathic LBBB to LBBB-CMP diagnosis and treatment.Heart Vessels. 2025 Jan;40(1):62-71. doi: 10.1007/s00380-024-02441-2. Epub 2024 Jul 22. Heart Vessels. 2025. PMID: 39039344
-
Abnormal Conduction-Induced Cardiomyopathy: JACC Review Topic of the Week.J Am Coll Cardiol. 2023 Mar 28;81(12):1192-1200. doi: 10.1016/j.jacc.2023.01.040. J Am Coll Cardiol. 2023. PMID: 36948737 Free PMC article. Review.
-
2023 HRS/APHRS/LAHRS guideline on cardiac physiologic pacing for the avoidance and mitigation of heart failure.Heart Rhythm. 2023 Sep;20(9):e17-e91. doi: 10.1016/j.hrthm.2023.03.1538. Epub 2023 May 20. Heart Rhythm. 2023. PMID: 37283271 Free PMC article.
References
-
- Eriksson P, Hansson PO, Eriksson H, Dellborg M. Bundle‐branch block in a general male population: the study of men born 1913. Circulation. 1998;98:2494‐2500. - PubMed
-
- Eriksson P, Wilhelmsen L, Rosengren A. Bundle‐branch block in middle‐aged men: risk of complications and death over 28 years. Eur Heart J. 2005;26:2300. - PubMed
-
- Fahy GJ, Pinski SL, Miller DP, et al. Natural history of isolated bundle branch block. Am J Cardiol. 1996;77:1185‐1190. - PubMed
-
- Imanishi R, Seto S, Ichimaru S, Nakashima E, Yano K, Akahoshi M. Prognostic significance of incident complete left bundle branch block observed over a 40‐year period. Am J Cardiol. 2006;98:644‐648. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
