

Cardiovascular responses to rhythmic handgrip exercise in heart failure with preserved ejection fraction
- PMID: 32940557
- PMCID: PMC7792839
- DOI: 10.1152/japplphysiol.00468.2020
Cardiovascular responses to rhythmic handgrip exercise in heart failure with preserved ejection fraction
Abstract
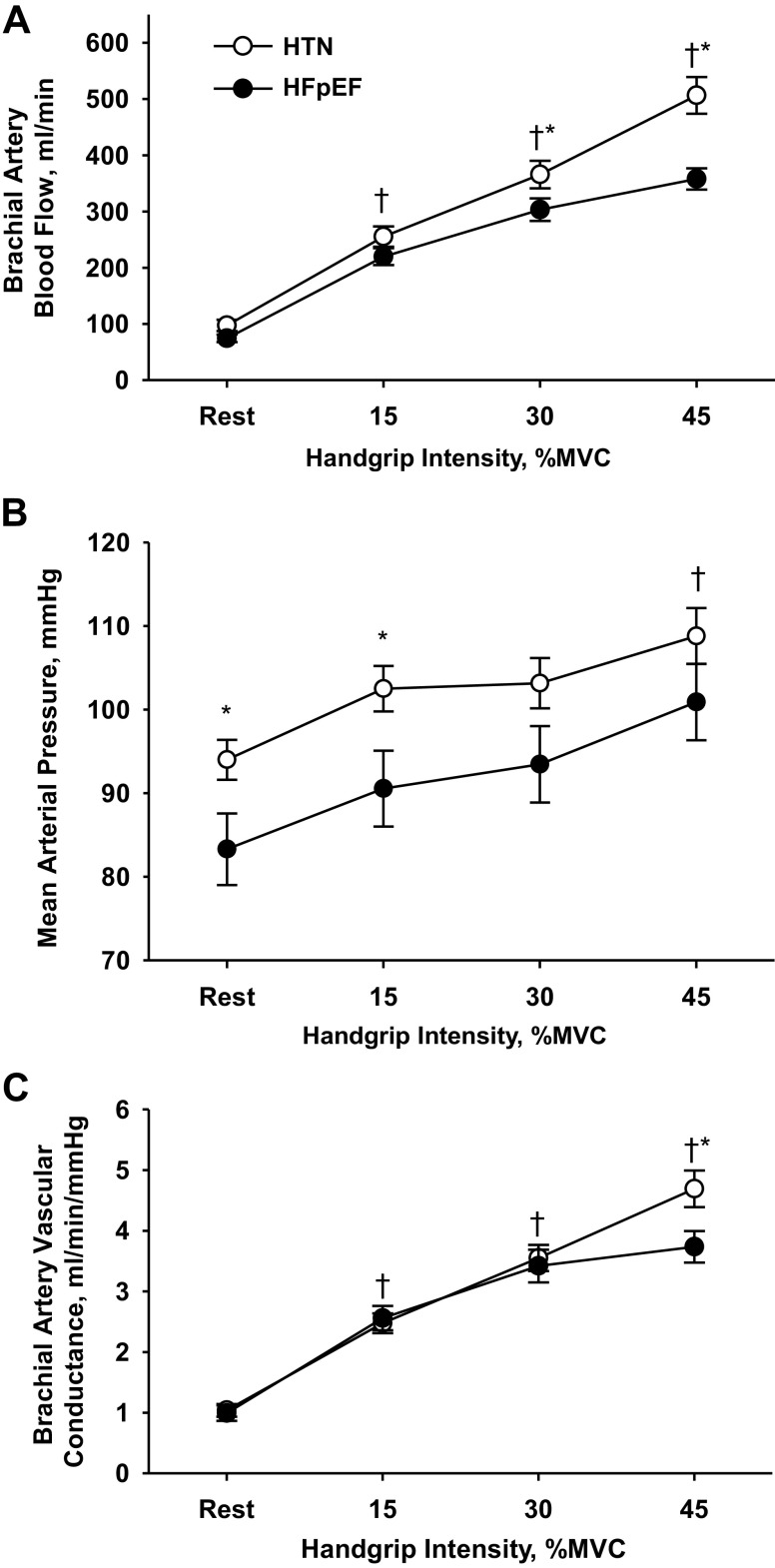
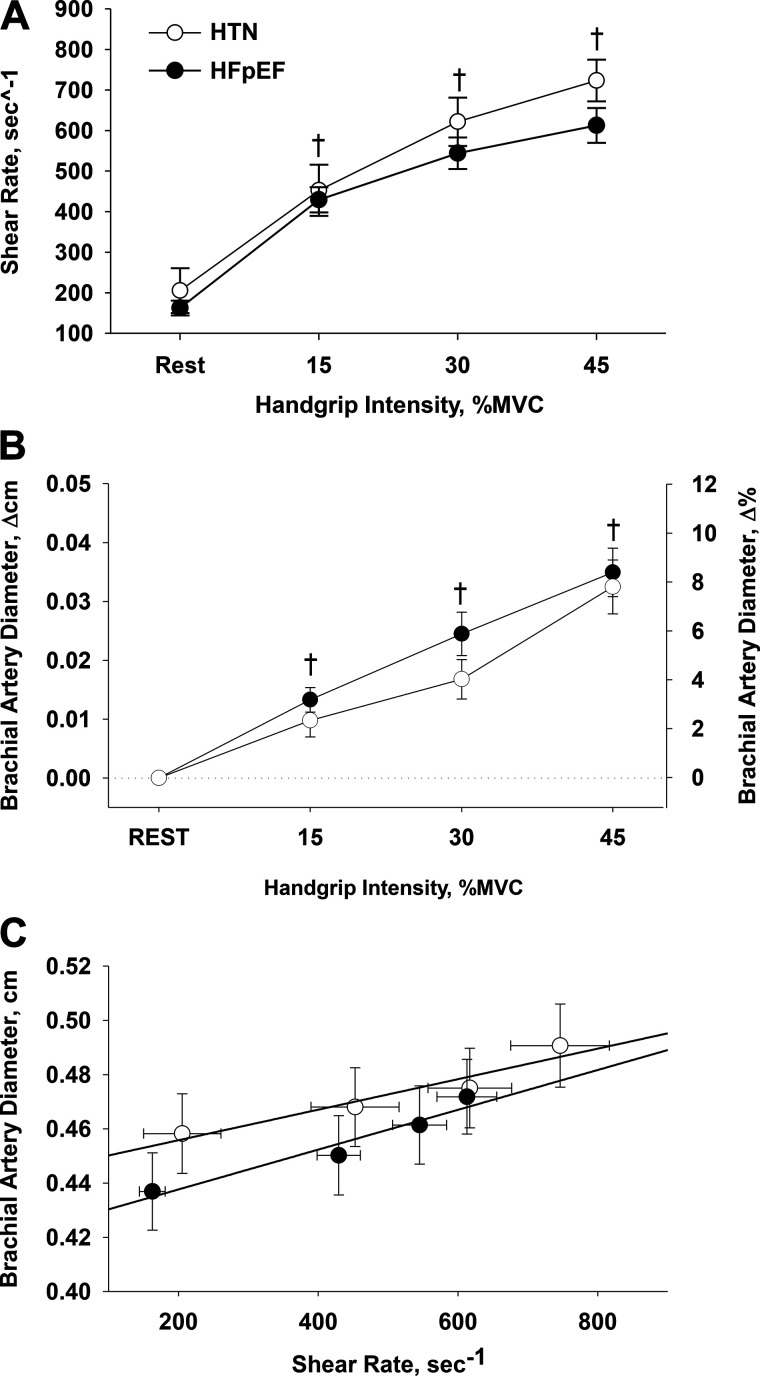
Although the contribution of noncardiac complications to the pathophysiology of heart failure with preserved ejection fraction (HFpEF) have been increasingly recognized, disease-related changes in peripheral vascular control remain poorly understood. We utilized small muscle mass handgrip exercise to concomitantly evaluate exercising muscle blood flow and conduit vessel endothelium-dependent vasodilation in individuals with HFpEF (n = 25) compared with hypertensive controls (HTN) (n = 25). Heart rate (HR), stroke volume (SV), cardiac output (CO), mean arterial pressure (MAP), brachial artery blood velocity, and brachial artery diameter were assessed during progressive intermittent handgrip (HG) exercise [15-30-45% maximal voluntary contraction (MVC)]. Forearm blood flow (FBF) and vascular conductance (FVC) were determined to quantify the peripheral hemodynamic response to HG exercise, and changes in brachial artery diameter were evaluated to assess endothelium-dependent vasodilation. HR, SV, and CO were not different between groups across exercise intensities. However, although FBF was not different between groups at the lowest exercise intensity, FBF was significantly lower (20-40%) in individuals with HFpEF at the two higher exercise intensities (30% MVC: 229 ± 8 versus 274 ± 23 ml/min; 45% MVC: 283 ± 17 versus 399 ± 34 ml/min, HFpEF versus HTN). FVC was not different between groups at 15 and 30% MVC but was ∼20% lower in HFpEF at the highest exercise intensity. Brachial artery diameter increased across exercise intensities in both HFpEF and HTN, with no difference between groups. These findings demonstrate an attenuation in muscle blood flow during exercise in HFpEF in the absence of disease-related changes in central hemodynamics or endothelial function.NEW & NOTEWORTHY The current study identified, for the first time, an attenuation in exercising muscle blood flow during handgrip exercise in individuals with heart failure with preserved ejection fraction (HFpEF) compared with overweight individuals with hypertension, two of the most common comorbidities associated with HFpEF. These decrements in exercise hyperemia cannot be attributed to disease-related changes in central hemodynamics or endothelial function, providing additional evidence for disease-related vascular dysregulation, which may be a predominant contributor to exercise intolerance in individuals with HFpEF.
Keywords: blood flow; endothelium-dependent vasodilation; exercise hyperemia; small muscle mass handgrip exercise.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
References
-
- Akiyama E, Sugiyama S, Matsuzawa Y, Konishi M, Suzuki H, Nozaki T, Ohba K, Matsubara J, Maeda H, Horibata Y, Sakamoto K, Sugamura K, Yamamuro M, Sumida H, Kaikita K, Iwashita S, Matsui K, Kimura K, Umemura S, Ogawa H. Incremental prognostic significance of peripheral endothelial dysfunction in patients with heart failure with normal left ventricular ejection fraction. J Am Coll Cardiol 60: 1778–1786, 2012. doi:10.1016/j.jacc.2012.07.036. - DOI - PubMed
-
- Altun I, Oz F, Arkaya SC, Altun I, Bilge AK, Umman B, Turkoglu UM. Effect of statins on endothelial function in patients with acute coronary syndrome: a prospective study using adhesion molecules and flow-mediated dilatation. J Clin Med Res 6: 354–361, 2014. doi:10.14740/jocmr1863w. - DOI - PMC - PubMed
-
- Barrett-O’Keefe Z, Lee JF, Berbert A, Witman MA, Nativi-Nicolau J, Stehlik J, Richardson RS, Wray DW. Hemodynamic responses to small muscle mass exercise in heart failure patients with reduced ejection fraction. Am J Physiol Heart Circ Physiol 307: H1512–H1520, 2014. doi:10.1152/ajpheart.00527.2014. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- I01RX001311/VA/VA/United States
- T32 HL139451/HL/NHLBI NIH HHS/United States
- I21RX001433/VA/VA/United States
- T32HL139451/NH/NIH HHS/United States
- I01 RX000182/RX/RRD VA/United States
- 14SDG18850039/AHA/American Heart Association-American Stroke Association/United States
- R01 HL118313/HL/NHLBI NIH HHS/United States
- I01RX002323/VA/VA/United States
- I21 RX001433/RX/RRD VA/United States
- IK2RX001215/VA/VA/United States
- I01RX001697/VA/VA/United States
- IK2 RX001215/RX/RRD VA/United States
- I01 RX001311/RX/RRD VA/United States
- R01HL118313/NH/NIH HHS/United States
- I01 RX002323/RX/RRD VA/United States
- I01 RX001697/RX/RRD VA/United States
LinkOut - more resources
Full Text Sources
Medical