

Pain management in patients with chronic kidney disease and end-stage kidney disease
- PMID: 32941189
- PMCID: PMC7753951
- DOI: 10.1097/MNH.0000000000000646
Pain management in patients with chronic kidney disease and end-stage kidney disease
Abstract
Purpose of review: This review evaluates current recommendations for pain management in chronic kidney disease (CKD) and end-stage kidney disease (ESKD) with a specific focus on evidence for opioid analgesia, including the partial agonist, buprenorphine.
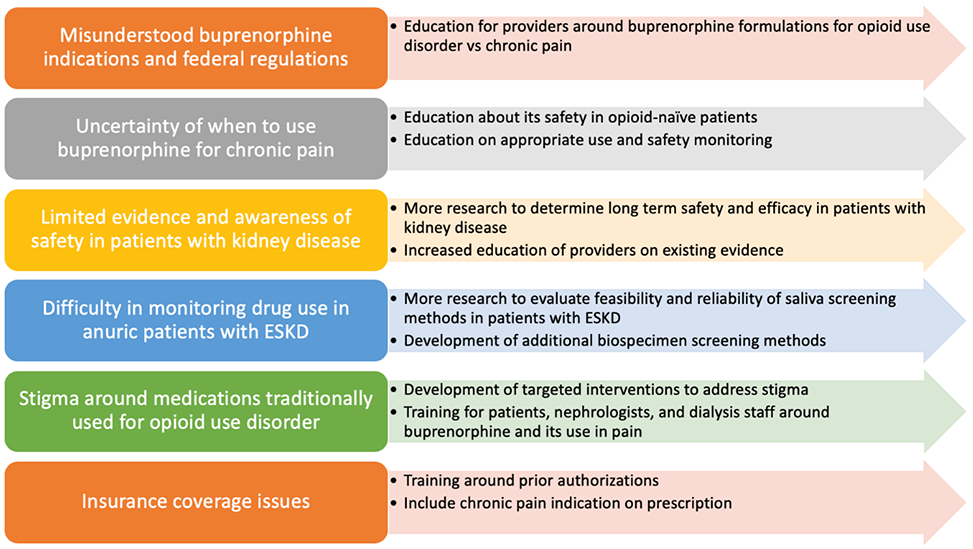
Recent findings: Recent evidence supports the use of physical activity and other nonpharmacologic therapies, either alone or with pharmacological therapies, for pain management. Nonopioid analgesics, including acetaminophen, topical analgesics, gabapentinoids, serotonin-norepinephrine reuptake inhibitors, and TCA may be considered based on pain cause and type, with careful dose considerations in kidney disease. NSAIDs may be used in CKD and ESKD for short durations with careful monitoring. Opioid use should be minimized and reserved for patients who have failed other therapies. Opioids have been associated with increased adverse events in this population, and thus should be used cautiously after risk/benefit discussion with the patient. Opioids that are safer to use in kidney disease include oxycodone, hydromorphone, fentanyl, methadone, and buprenorphine. Buprenorphine appears to be a promising and safer option due to its partial agonism at the mu opioid receptor.
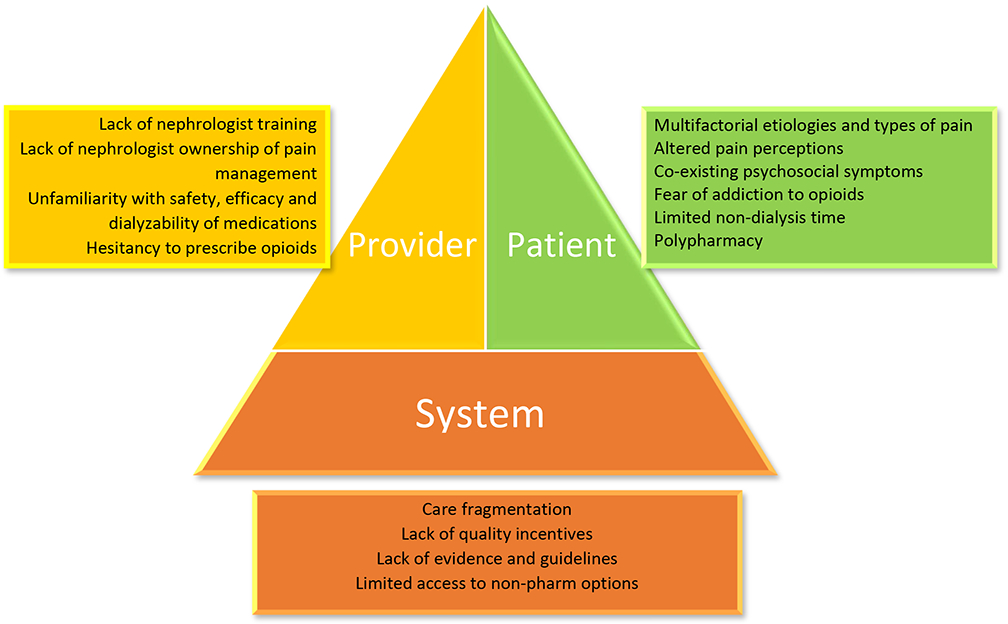
Summary: Pain is poorly managed in patients with kidney disease. Nonpharmacological and nonopioid analgesics should be first-line approaches for pain management. Opioid use should be minimized with careful monitoring and dose adjustment.
Conflict of interest statement
Conflicts of interest: Laura M. Dember receives compensation for her role as Deputy Editor of the American Journal of Kidney Diseases and consulting fees from Merck.
Figures
References
-
- Mercadante S, Ferrantelli A, Tortorici C, et al. Incidence of Chronic Pain in Patients with End-Stage Renal Disease on Dialysis. J Pain Symptom Manage [Internet]. 2005. October;30(4):302–4. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0885392405004343 - PubMed
-
- Davison SN. Clinical Pharmacology Considerations in Pain Management in Patients with Advanced Kidney Failure. Clin J Am Soc Nephrol [Internet]. 2019;14(6):917–31. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30833302 - PMC - PubMed
-
- Davison SN, Jhangri GS. Impact of Pain and Symptom Burden on the Health-Related Quality of Life of Hemodialysis Patients. J Pain Symptom Manage [Internet]. 2010. March;39(3):477–85. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0885392410000898 - PubMed
-
- Harris TJ, Nazir R, Khetpal P, et al. Pain, sleep disturbance and survival in hemodialysis patients. Nephrol Dial Transplant [Internet]. 2012. February 1;27(2):758–65. Available from: https://academic.oup.com/ndt/article-lookup/doi/10.1093/ndt/gfr355 - DOI - PMC - PubMed
-
- Weisbord SD, Mor MK, Sevick MA, et al. Associations of Depressive Symptoms and Pain with Dialysis Adherence, Health Resource Utilization, and Mortality in Patients Receiving Chronic Hemodialysis. Clin J Am Soc Nephrol [Internet]. 2014. September 5;9(9):1594–602. Available from: http://cjasn.asnjournals.org/lookup/doi/10.2215/CJN.00220114 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
