

Combined associations of body mass index and adherence to a Mediterranean-like diet with all-cause and cardiovascular mortality: A cohort study
- PMID: 32941436
- PMCID: PMC7497998
- DOI: 10.1371/journal.pmed.1003331
Combined associations of body mass index and adherence to a Mediterranean-like diet with all-cause and cardiovascular mortality: A cohort study
Abstract
Background: It is unclear whether the effect on mortality of a higher body mass index (BMI) can be compensated for by adherence to a healthy diet and whether the effect on mortality by a low adherence to a healthy diet can be compensated for by a normal weight. We aimed to evaluate the associations of BMI combined with adherence to a Mediterranean-like diet on all-cause and cardiovascular disease (CVD) mortality.
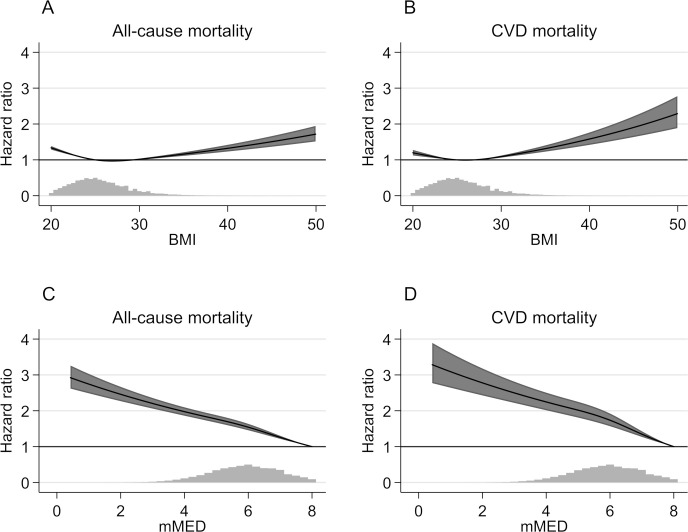
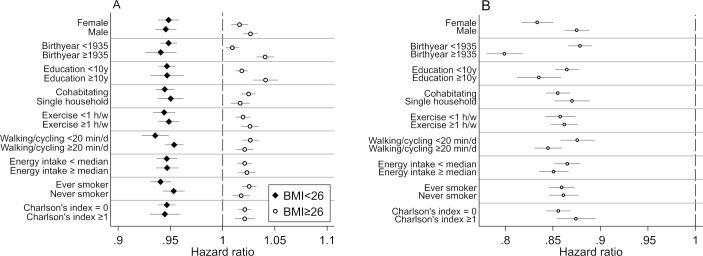
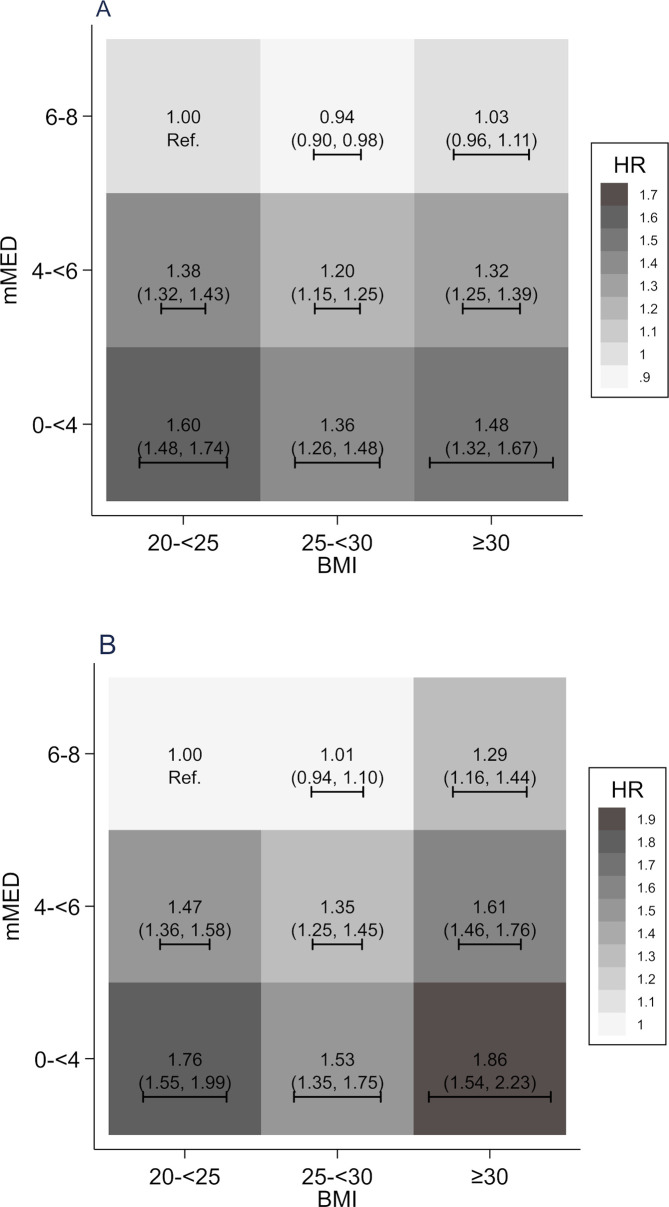
Methods and findings: Our longitudinal cohort design included the Swedish Mammography Cohort (SMC) and the Cohort of Swedish Men (COSM) (1997-2017), with a total of 79,003 women (44%) and men (56%) and a mean baseline age of 61 years. BMI was categorized into normal weight (20-24.9 kg/m2), overweight (25-29.9 kg/m2), and obesity (30+ kg/m2). Adherence to a Mediterranean-like diet was assessed by means of the modified Mediterranean-like diet (mMED) score, ranging from 0 to 8; mMED was classified into 3 categories (0 to <4, 4 to <6, and 6-8 score points), forming a total of 9 BMI × mMED combinations. We identified mortality by use of national Swedish registers. Cox proportional hazard models with time-updated information on exposure and covariates were used to calculate the adjusted hazard ratios (HRs) of mortality with their 95% confidence intervals (CIs). Our HRs were adjusted for age, baseline educational level, marital status, leisure time physical exercise, walking/cycling, height, energy intake, smoking habits, baseline Charlson's weighted comorbidity index, and baseline diabetes mellitus. During up to 21 years of follow-up, 30,389 (38%) participants died, corresponding to 22 deaths per 1,000 person-years. We found the lowest HR of all-cause mortality among overweight individuals with high mMED (HR 0.94; 95% CI 0.90, 0.98) compared with those with normal weight and high mMED. Using the same reference, obese individuals with high mMED did not experience significantly higher all-cause mortality (HR 1.03; 95% CI 0.96-1.11). In contrast, compared with those with normal weight and high mMED, individuals with a low mMED had a high mortality despite a normal BMI (HR 1.60; 95% CI 1.48-1.74). We found similar estimates among women and men. For CVD mortality (12,064 deaths) the findings were broadly similar, though obese individuals with high mMED retained a modestly increased risk of CVD death (HR 1.29; 95% CI 1.16-1.44) compared with those with normal weight and high mMED. A main limitation of the present study is the observational design with self-reported lifestyle information with risk of residual or unmeasured confounding (e.g., genetic liability), and no causal inferences can be made based on this study alone.
Conclusions: These findings suggest that diet quality modifies the association between BMI and all-cause mortality in women and men. A healthy diet may, however, not completely counter higher CVD mortality related to obesity.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Global BMIMC, Di Angelantonio E, Bhupathiraju Sh N, Wormser D, Gao P, Kaptoge S, et al. Body-mass index and all-cause mortality: individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet. 2016;388(10046):776–86. 10.1016/S0140-6736(16)30175-1 . - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
