

Interventions for treatment of COVID-19: A living systematic review with meta-analyses and trial sequential analyses (The LIVING Project)
- PMID: 32941437
- PMCID: PMC7498193
- DOI: 10.1371/journal.pmed.1003293
Interventions for treatment of COVID-19: A living systematic review with meta-analyses and trial sequential analyses (The LIVING Project)
Erratum in
-
Correction: Interventions for treatment of COVID-19: A living systematic review with meta-analyses and trial sequential analyses (The LIVING Project).PLoS Med. 2020 Dec 29;17(12):e1003517. doi: 10.1371/journal.pmed.1003517. eCollection 2020 Dec. PLoS Med. 2020. PMID: 33373360 Free PMC article.
Abstract
Background: Coronavirus disease 2019 (COVID-19) is a rapidly spreading disease that has caused extensive burden to individuals, families, countries, and the world. Effective treatments of COVID-19 are urgently needed.
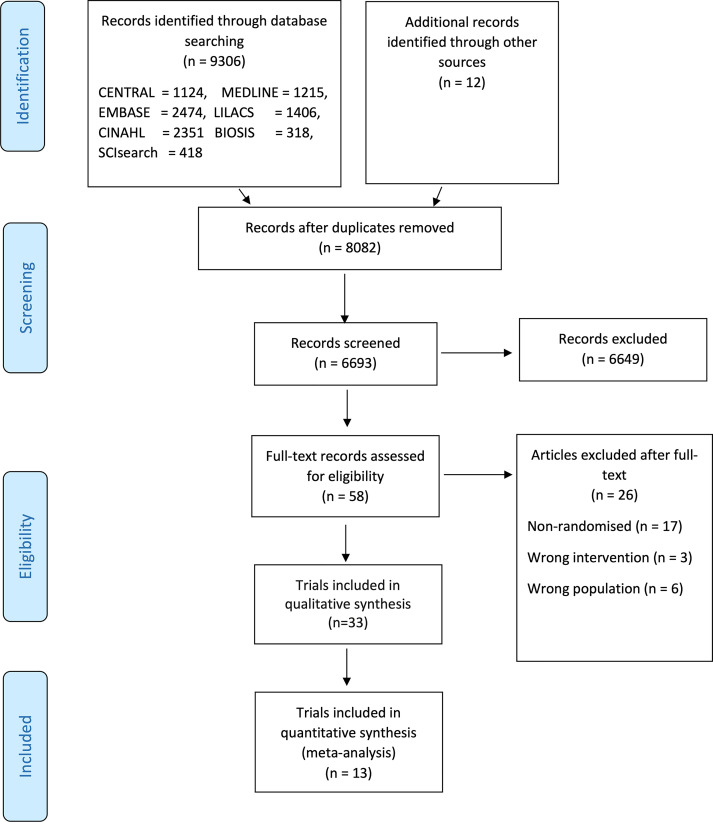
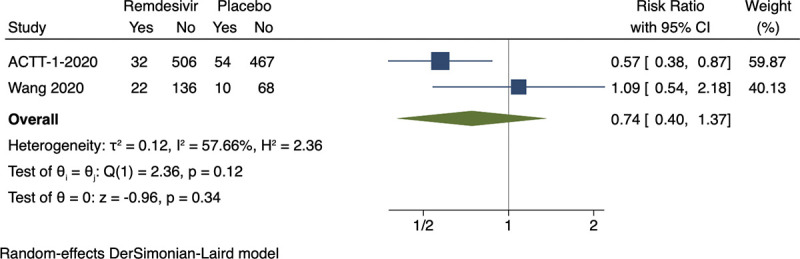
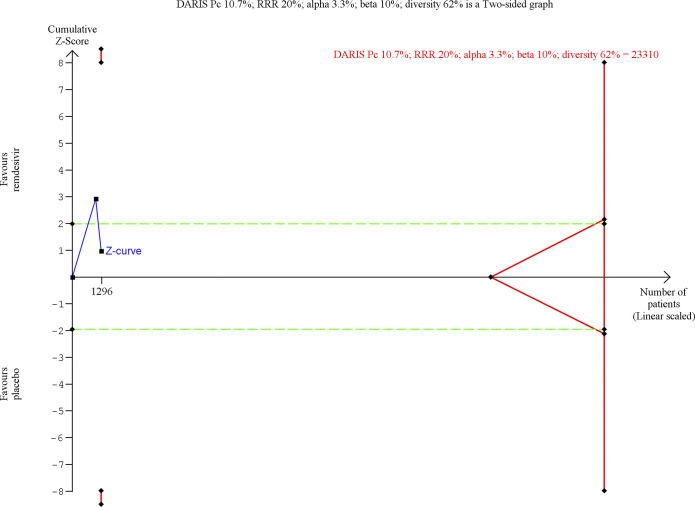
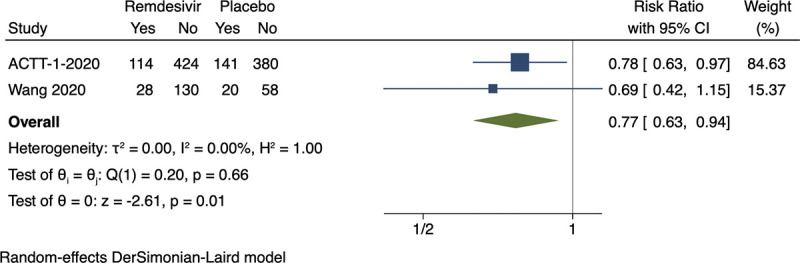
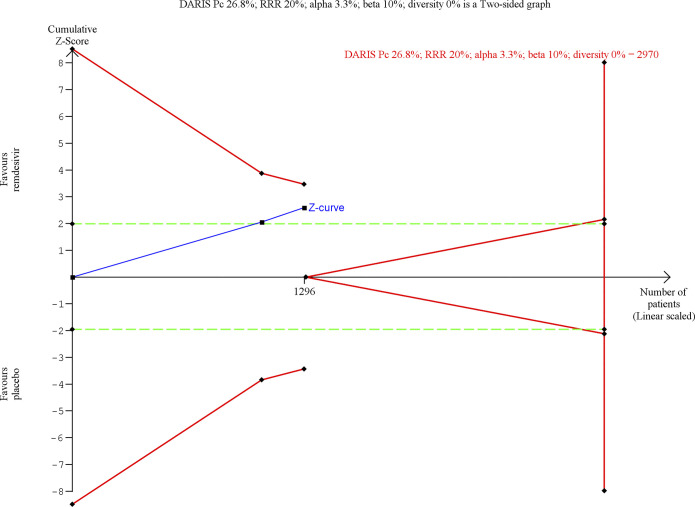
Methods and findings: This is the first edition of a living systematic review of randomized clinical trials comparing the effects of all treatment interventions for participants in all age groups with COVID-19. We planned to conduct aggregate data meta-analyses, trial sequential analyses, network meta-analysis, and individual patient data meta-analyses. Our systematic review is based on Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) and Cochrane guidelines, and our 8-step procedure for better validation of clinical significance of meta-analysis results. We performed both fixed-effect and random-effects meta-analyses. Primary outcomes were all-cause mortality and serious adverse events. Secondary outcomes were admission to intensive care, mechanical ventilation, renal replacement therapy, quality of life, and nonserious adverse events. We used Grading of Recommendations Assessment, Development and Evaluation (GRADE) to assess the certainty of evidence. We searched relevant databases and websites for published and unpublished trials until August 7, 2020. Two reviewers independently extracted data and assessed trial methodology. We included 33 randomized clinical trials enrolling a total of 13,312 participants. All trials were at overall high risk of bias. We identified one trial randomizing 6,425 participants to dexamethasone versus standard care. This trial showed evidence of a beneficial effect of dexamethasone on all-cause mortality (rate ratio 0.83; 95% confidence interval [CI] 0.75-0.93; p < 0.001; low certainty) and on mechanical ventilation (risk ratio [RR] 0.77; 95% CI 0.62-0.95; p = 0.021; low certainty). It was possible to perform meta-analysis of 10 comparisons. Meta-analysis showed no evidence of a difference between remdesivir versus placebo on all-cause mortality (RR 0.74; 95% CI 0.40-1.37; p = 0.34, I2 = 58%; 2 trials; very low certainty) or nonserious adverse events (RR 0.94; 95% CI 0.80-1.11; p = 0.48, I2 = 29%; 2 trials; low certainty). Meta-analysis showed evidence of a beneficial effect of remdesivir versus placebo on serious adverse events (RR 0.77; 95% CI 0.63-0.94; p = 0.009, I2 = 0%; 2 trials; very low certainty) mainly driven by respiratory failure in one trial. Meta-analyses and trial sequential analyses showed that we could exclude the possibility that hydroxychloroquine versus standard care reduced the risk of all-cause mortality (RR 1.07; 95% CI 0.97-1.19; p = 0.17; I2 = 0%; 7 trials; low certainty) and serious adverse events (RR 1.07; 95% CI 0.96-1.18; p = 0.21; I2 = 0%; 7 trials; low certainty) by 20% or more, and meta-analysis showed evidence of a harmful effect on nonserious adverse events (RR 2.40; 95% CI 2.01-2.87; p < 0.00001; I2 = 90%; 6 trials; very low certainty). Meta-analysis showed no evidence of a difference between lopinavir-ritonavir versus standard care on serious adverse events (RR 0.64; 95% CI 0.39-1.04; p = 0.07, I2 = 0%; 2 trials; very low certainty) or nonserious adverse events (RR 1.14; 95% CI 0.85-1.53; p = 0.38, I2 = 75%; 2 trials; very low certainty). Meta-analysis showed no evidence of a difference between convalescent plasma versus standard care on all-cause mortality (RR 0.60; 95% CI 0.33-1.10; p = 0.10, I2 = 0%; 2 trials; very low certainty). Five single trials showed statistically significant results but were underpowered to confirm or reject realistic intervention effects. None of the remaining trials showed evidence of a difference on our predefined outcomes. Because of the lack of relevant data, it was not possible to perform other meta-analyses, network meta-analysis, or individual patient data meta-analyses. The main limitation of this living review is the paucity of data currently available. Furthermore, the included trials were all at risks of systematic errors and random errors.
Conclusions: Our results show that dexamethasone and remdesivir might be beneficial for COVID-19 patients, but the certainty of the evidence was low to very low, so more trials are needed. We can exclude the possibility of hydroxychloroquine versus standard care reducing the risk of death and serious adverse events by 20% or more. Otherwise, no evidence-based treatment for COVID-19 currently exists. This review will continuously inform best practice in treatment and clinical research of COVID-19.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization. Novel Coronavirus (2019-nCOV). Situation Report 51. 2020. [cited 2020 Aug 7]. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/2...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
