

The proportion of endometrial tumours associated with Lynch syndrome (PETALS): A prospective cross-sectional study
- PMID: 32941469
- PMCID: PMC7497985
- DOI: 10.1371/journal.pmed.1003263
The proportion of endometrial tumours associated with Lynch syndrome (PETALS): A prospective cross-sectional study
Abstract
Background: Lynch syndrome (LS) predisposes to endometrial cancer (EC), colorectal cancer, and other cancers through inherited pathogenic variants affecting mismatch-repair (MMR) genes. Diagnosing LS in women with EC can reduce subsequent cancer mortality through colonoscopic surveillance and aspirin chemoprevention; it also enables cascade testing of relatives. A growing consensus supports LS screening in EC; however, the expected proportion of test positives, and optimal testing strategy is uncertain. Previous studies from insurance-based healthcare systems were limited by narrow selection criteria, failure to apply reference standard tests consistently, and poor conversion to definitive testing. The aim of this study was to establish the prevalence of LS and the diagnostic accuracy of LS testing strategies in an unselected EC population.
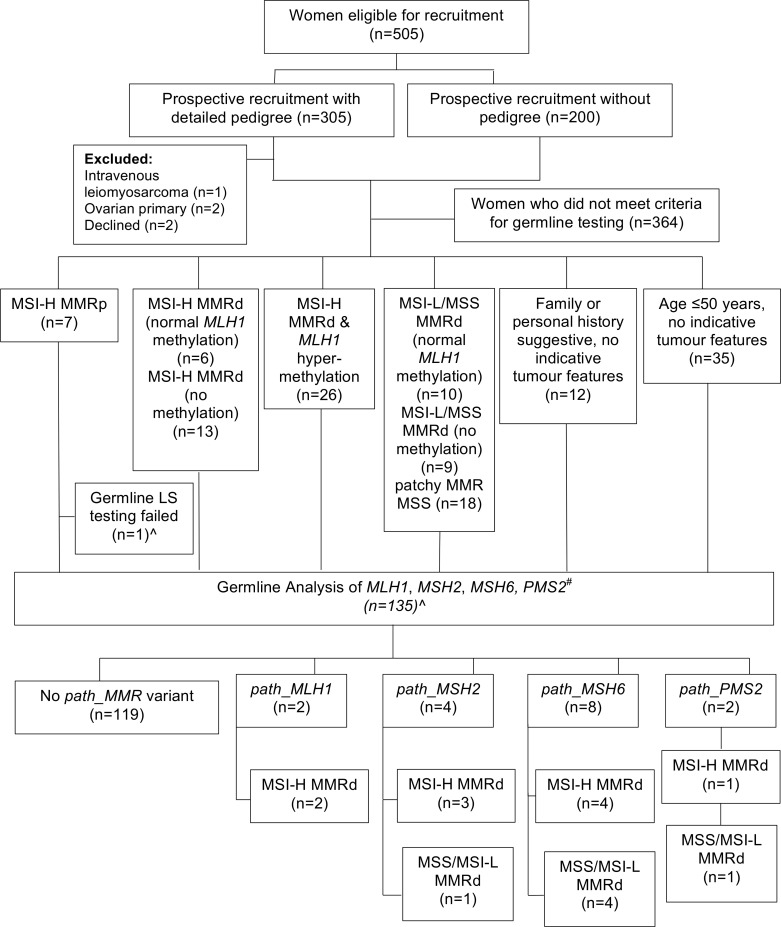
Methods and findings: This was a prospective cross-sectional study carried out at a large United Kingdom gynaecological cancer centre between October 2015 and January 2017. Women diagnosed with EC or atypical hyperplasia (AH) were offered LS testing. Tumours underwent MMR immunohistochemistry (IHC), microsatellite instability (MSI), and targeted MLH1-methylation testing. Women <50 years, with strong family histories and/or indicative tumour molecular features, underwent MMR germline sequencing. Somatic MMR sequencing was performed when indicative molecular features were unexplained by LS or MLH1-hypermethylation. The main outcome measures were the prevalence of LS in an unselected EC population and the diagnostic accuracy of clinical and tumour testing strategies for risk stratifying women with EC for MMR germline sequencing. In total, 500 women participated in the study; only 2 (<1%) declined. Germline sequencing was indicated and conducted for 136 and 135 women, respectively. A total of 16/500 women (3.2%, 95% CI 1.8% to 5.1%) had LS, and 11 more (2.2%) had MMR variants of uncertain significance. Restricting testing to age <50 years, indicative family history (revised Bethesda guidelines or Amsterdam II criteria) or endometrioid histology alone would have missed 9/16 (56%), 8/13 (62%) or 9/13 (69%), and 5/16 (31%) cases of LS, respectively. In total 132/500 tumours were MMR deficient by IHC of which 83/132 (63%) had MLH1-hypermethylation, and 16/49 (33%) of the remaining patients had LS (16/132 with MMR deficiency, 12%). MMR-IHC with targeted MLH1-methylation testing was more discriminatory for LS than MSI with targeted methylation testing, with 100% versus 56.3% (16/16 versus 9/16) sensitivity (p = 0.016) and equal 97.5% (468/484) specificity; 64% MSI-H and 73% MMR deficient tumours unexplained by LS or MLH1-hypermethylation had somatic MMR mutations. The main limitation of the study was failure to conduct MMR germline sequencing for the whole study population, which means that the sensitivity and specificity of tumour triage strategies for LS detection may be overestimated, although the risk of LS in women with no clinical or tumour predictors is expected to be extremely low.
Conclusions: In this study, we observed that age, family history, and histology are imprecise clinical correlates of LS-EC. IHC outperformed MSI for tumour triage and reliably identified both germline and somatic MMR mutations. The 3.2% proportion of LS-EC is similar to colorectal cancer, supporting unselected screening of EC for LS.
Conflict of interest statement
We have read the journal's policy and the authors of this manuscript have the following competing interests: IMF is an Honorary Medical Advisor to Lynch Syndrome UK and reports support from St Vincent’s University Hospital (Dublin), Impact Genetics (Bowmanville, Ontario, Canada), and Ambry Genetics (Aliso Viejo, CA, USA), for travel, outside the submitted work. Other authors declare that no competing interests exist.
Figures
References
-
- Møller P, Seppälä T, Bernstein I, Holinski-Feder E, Sala P, Evans DG, et al. Cancer incidence and survival in Lynch syndrome patients receiving colonoscopic and gynaecological surveillance: first report from the prospective Lynch syndrome database. Gut. 2017;66: 464–472. 10.1136/gutjnl-2015-309675 - DOI - PMC - PubMed
-
- Lu KH, Dinh M, Kohlmann W, Watson P, Green J, Syngal S, et al. Gynecologic Cancer as a “Sentinel Cancer” for Women With Hereditary Nonpolyposis Colorectal Cancer Syndrome. Obstetrics and gynecology. 2005;105: 569–574. 10.1097/01.aog.0000154885.44002.ae - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
