

Gastric adenomas and their management in familial adenomatous polyposis
- PMID: 32942317
- PMCID: PMC8315898
- DOI: 10.1055/a-1265-2716
Gastric adenomas and their management in familial adenomatous polyposis
Abstract
Background: Patients with familial adenomatous polyposis (FAP) are at increased risk of developing gastric adenomas. There is limited understanding of their clinical course and no consensus on management. We reviewed the management of gastric adenomas in patients with FAP from two centers.
Methods: Patients with FAP and histologically confirmed gastric adenomas were identified between 1997 and 2018. Patient demographics, adenoma characteristics, and management/surveillance outcomes were collected.
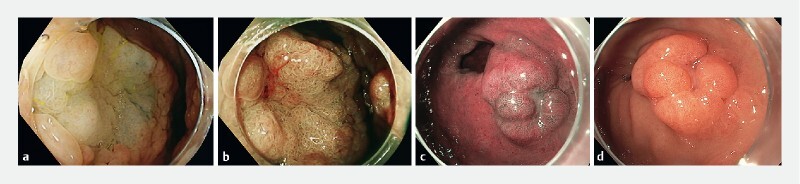
Results: Of 726 patients with FAP, 104 (14 %; 49 female) were diagnosed with gastric adenomas at a median age of 47 years (range 19 - 80). The median size of gastric adenomas was 6 mm (range 1.5 - 50); 64 (62 %) patients had adenomas located distally to the incisura. Five patients (5 %) had gastric adenomas demonstrating high-grade dysplasia (HGD) on initial diagnosis, distributed equally within the stomach. The risk of HGD was associated with adenoma size (P = 0.04). Of adenomas > 20 mm, 33 % contained HGD. Two patients had gastric cancer at initial gastric adenoma diagnosis. A total of 63 patients (61 %) underwent endoscopic therapy for gastric adenomas. Complications occurred in three patients (5 %) and two (3 %) had recurrence, all following piecemeal resection of large (30 - 50 mm) lesions. Three patients were diagnosed with gastric cancer at median follow-up of 66 months (range 66 - 115) after initial diagnosis.
Conclusions: We observed gastric adenomas in 14 % of patients with FAP. Of these, 5 % contained HGD; risk of HGD correlated with adenoma size. Endoscopic resection was feasible, with few complications and low recurrence rates, but did not completely eliminate the cancer risk.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Prof. Dekker has received a research grant and equipment loans from FujiFilm. She has also received honoraria for consultancy work for FujiFilm, Olympus, Tillots, GI Supply, and CPP-FAP, and speaker fees from Olympus, Roche, and GI supply. All other authors declare that they have no conflicts of interest.
Figures
Comment in
-
Author commentary on Isabel Martin et al.Endoscopy. 2021 Aug;53(8):v39. doi: 10.1055/a-1326-4948. Epub 2021 Jul 27. Endoscopy. 2021. PMID: 34315180 No abstract available.
References
-
- Kinzler K, Nilbert M, Su L et al.Identification of FAP locus genes from chromosome 5q21. Science. 1991;253:661–665. - PubMed
-
- Bisgaard M, Fenger K, Bulow S et al.Familial adenomatous polyposis (FAP): frequency, penetrance and mutation rate. Hum Mutat. 1994;3:121–125. - PubMed
-
- Arvanitis M, Jagelman D. Mortality in patients with familial adenomatous polyposis. Dis Colon Rectum. 1990;33:639–642. - PubMed
-
- Nugent K P, Spigelman A D, Phillips R KS. Life expectancy after colectomy and ileorectal anastomosis for familial adenomatous polyposis. Dis Colon Rectum. 1993;36:1059–1062. - PubMed
-
- Ghorbanoghli Z, Bastiaansen B AJ, Langers A MJ et al.Extracolonic cancer risk in Dutch patients with APC (adenomatous polyposis coli)-associated polyposis. J Med Genet. 2018;55:11–14. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous