

Improving treatment decision-making in bipolar II disorder: a phase II randomised controlled trial of an online patient decision-aid
- PMID: 32943031
- PMCID: PMC7495840
- DOI: 10.1186/s12888-020-02845-0
Improving treatment decision-making in bipolar II disorder: a phase II randomised controlled trial of an online patient decision-aid
Abstract
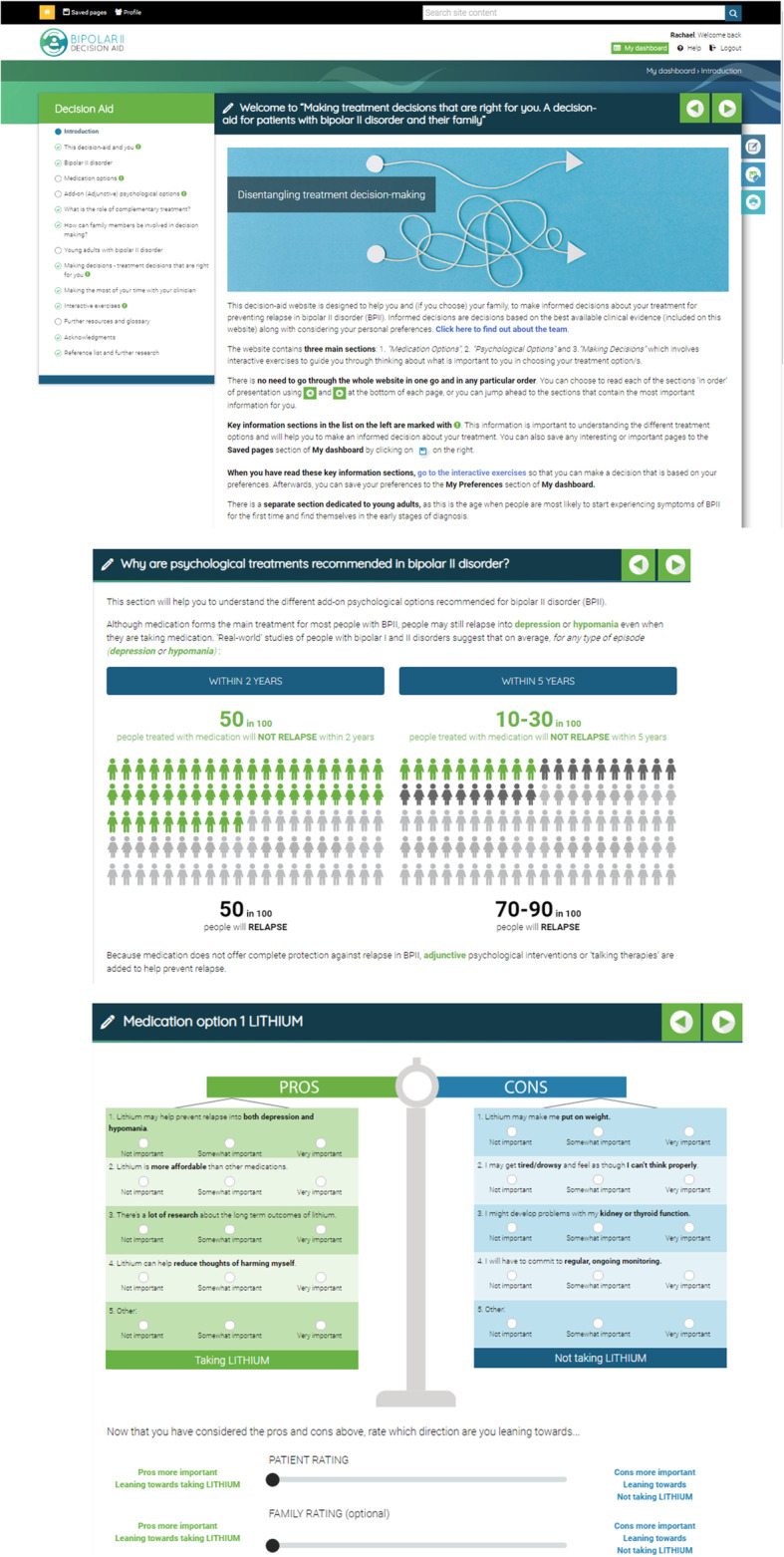
Background: Many patients with bipolar II disorder (BPII) prefer to be more informed and involved in their treatment decision-making than they currently are. Limited knowledge and involvement in one's treatment is also likely to compromise optimal BPII management. This Phase II RCT aimed to evaluate the acceptability, feasibility, and safety of a world-first patient decision-aid website (e-DA) to improve treatment decision-making regarding options for relapse prevention in BPII. The e-DA's potential efficacy in terms of improving quality of the decision-making process and quality of the decision made was also explored.
Methods: The e-DA was based on International Patient Decision-Aid Standards and developed via an iterative co-design process. Adults with BPII diagnosis (n = 352) were recruited through a specialist outpatient clinical service and the social media of leading mental health organisations. Participants were randomised (1:1) to receive standard information with/without the e-DA (Intervention versus Control). At baseline (T0), post-treatment decision (T1) and at 3 months' post-decision follow-up (T2), participants completed a series of validated and purpose-designed questionnaires. Self-report and analytics data assessed the acceptability (e.g., perceived ease-of-use, usefulness; completed by Intervention participants only), safety (i.e., self-reported bipolar and/or anxiety symptoms), and feasibility of using the e-DA (% accessed). For all participants, questionnaires assessed constructs related to quality of the decision-making process (e.g., decisional conflict) and quality of the decision made (e.g., knowledge of treatment options and outcomes).
Results: Intervention participants endorsed the e-DA as acceptable and feasible to use (82.1-94.6% item agreement); most self-reported using the e-DA either selectively (51.8%; relevant sections only) or thoroughly (34%). Exploratory analyses indicated the e-DA's potential efficacy to improve decision-making quality; most between-group standardised mean differences (SMD) were small-to-moderate. The largest potential effects were detected for objective treatment knowledge (- 0.69, 95% CIs - 1.04, - 0.33 at T1; and - 0.57, 95% CIs - 0.99,-0.14 at T2), decisional regret at T2 (0.42, 95% CIs 0.01, 0.84), preparation for decision-making at T1 (- 0.44, 95% CIs - 0.81, - 0.07), and the Decisional Conflict Scale Uncertainty subscale (0.42, 95% CIs 0.08, 0.08) and Total (0.36, 95% CIs 0.30, 0.69) scores, with all SMDs favouring the Intervention over the Control conditions. Regarding safety, e-DA use was not associated with worse bipolar symptoms or anxiety.
Conclusion: The e-DA appears to be acceptable, feasible, safe and potentially efficacious at improving patients' decision-making about BPII treatment. Findings also support the future adoption of the e-DA into patient care for BPII to foster treatment decisions based on the best available evidence and patient preferences.
Trial registration: Australian New Zealand Clinical Trials Registry ACTRN12617000840381 (prospectively registered 07/06/2017).
Keywords: Bipolar II disorder; Decisional conflict; Informed choice; Patient decision aid; Patient involvement; Patient knowledge; Phase II randomised controlled trial; Relapse prevention; Shared decision-making; Treatment.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Yatham LN. Diagnosis and management of patients with bipolar II disorder. J Clin Psychiatry. 2005;66(Suppl 1):13–17. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
