

Using diagnostic stewardship to reduce rates, healthcare expenditures and accurately identify cases of hospital-onset Clostridioides difficile infection
- PMID: 32943129
- PMCID: PMC9215221
- DOI: 10.1017/ice.2020.375
Using diagnostic stewardship to reduce rates, healthcare expenditures and accurately identify cases of hospital-onset Clostridioides difficile infection
Abstract
Objective: Lack of judicious testing can result in the incorrect diagnosis of Clostridioides difficile infection (CDI), unnecessary CDI treatment, increased costs and falsely augmented hospital-acquired infection (HAI) rates. We evaluated facility-wide interventions used at the VA San Diego Healthcare System (VASDHS) to reduce healthcare-onset, healthcare-facility-associated CDI (HO-HCFA CDI), including the use of diagnostic stewardship with test ordering criteria.
Design: We conducted a retrospective study to assess the effectiveness of measures implemented to reduce the rate of HO-HCFA CDI at the VASDHS from fiscal year (FY)2015 to FY2018.
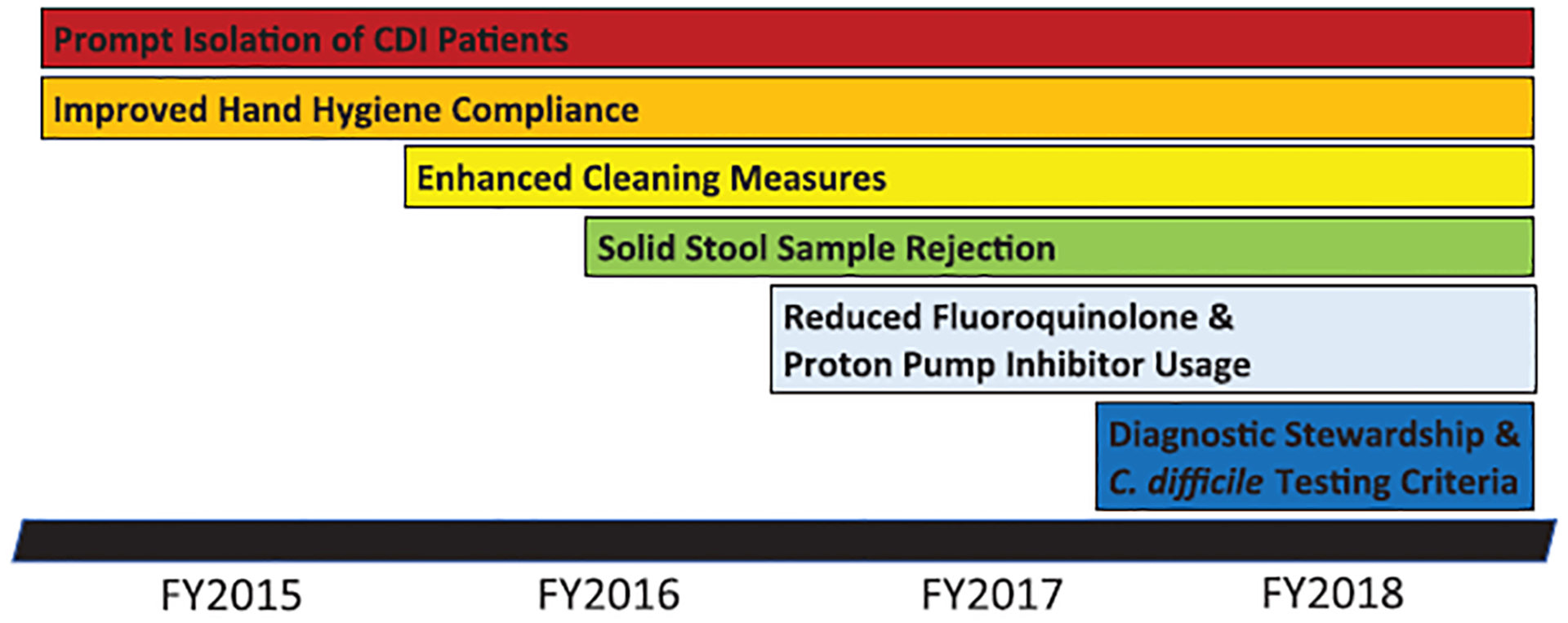
Interventions: Measures executed in a stepwise fashion included a hand hygiene initiative, prompt isolation of CDI patients, enhanced terminal room cleaning, reduction of fluoroquinolone and proton-pump inhibitor use, laboratory rejection of solid stool samples, and lastly diagnostic stewardship with C. difficile toxin B gene nucleic acid amplification testing (NAAT) criteria instituted in FY2018.
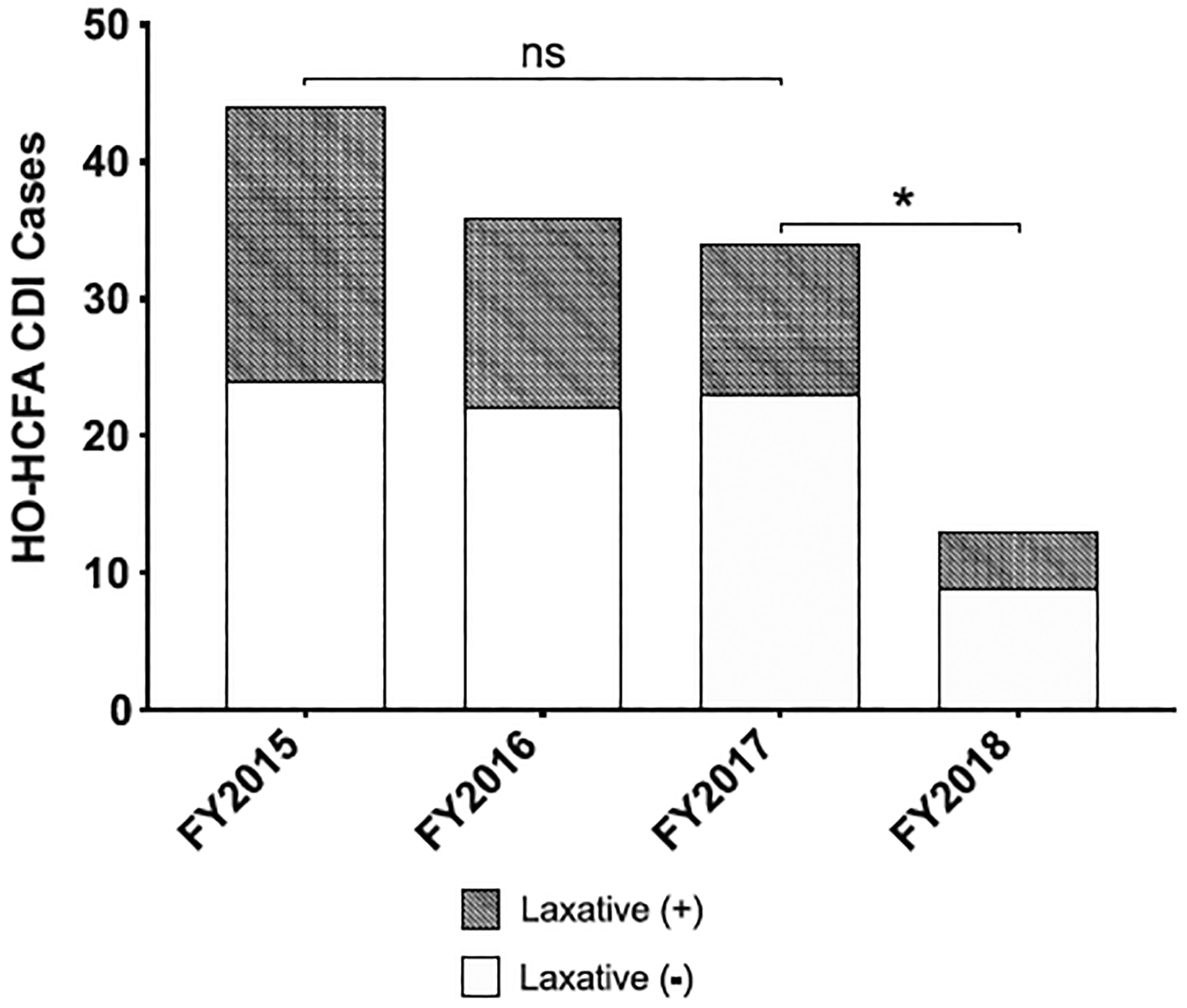
Results: From FY2015 to FY2018, 127 cases of HO-HCFA CDI were identified. All rate-reducing initiatives resulted in decreased HO-HCFA cases (from 44 to 13; P ≤ .05). However, the number of HO-HCFA cases (34 to 13; P ≤ .05), potential false-positive testing associated with colonization and laxative use (from 11 to 4), hospital days (from 596 to 332), CDI-related hospitalization costs (from $2,780,681 to $1,534,190) and treatment cost (from $7,158 vs $1,476) decreased substantially following the introduction of diagnostic stewardship with test criteria from FY2017 to FY2018.
Conclusions: Initiatives to decrease risk for CDI and diagnostic stewardship of C. difficile stool NAAT significantly reduced HO-HCFA CDI rates, detection of potential false-positives associated with laxative use, and lowered healthcare costs. Diagnostic stewardship itself had the most dramatic impact on outcomes observed and served as an effective tool in reducing HO-HCFA CDI rates.
Conflict of interest statement
Figures
Similar articles
-
Impact of mandatory nucleic acid amplification test (NAAT) testing approval on hospital-onset Clostridioides difficile infection (HO-CDI) rates: A diagnostic stewardship intervention.Infect Control Hosp Epidemiol. 2024 Jan;45(1):106-109. doi: 10.1017/ice.2023.92. Epub 2023 Jul 10. Infect Control Hosp Epidemiol. 2024. PMID: 37424227 Free PMC article.
-
Differences in time-to-testing and time-to-isolation between community-onset and hospital-onset Clostridioides difficile cases at a tertiary care VA medical center.Am J Infect Control. 2020 Oct;48(10):1148-1151. doi: 10.1016/j.ajic.2019.12.008. Epub 2020 Jan 3. Am J Infect Control. 2020. PMID: 31911067
-
Healthcare facility-onset, healthcare facility-associated Clostridioides difficile infection in Veterans with spinal cord injury and disorder.J Spinal Cord Med. 2020 Sep;43(5):642-652. doi: 10.1080/10790268.2019.1672953. Epub 2019 Oct 30. J Spinal Cord Med. 2020. PMID: 31663843 Free PMC article.
-
The impact of diagnostic stewardship interventions on Clostridiodes difficile test ordering practices and results.Clin Biochem. 2023 Jul;117:23-29. doi: 10.1016/j.clinbiochem.2022.03.009. Epub 2022 Apr 1. Clin Biochem. 2023. PMID: 35378064 Review.
-
Impact of hospital environmental cleaning with a potassium peroxymonosulphate-based environmental disinfectant and antimicrobial stewardship on the reduction of hospital-onset Clostridioides difficile infections.J Hosp Infect. 2022 Nov;129:181-188. doi: 10.1016/j.jhin.2022.06.018. Epub 2022 Jul 9. J Hosp Infect. 2022. PMID: 35820556 Review.
Cited by
-
Diagnostic stewardship to improve patient outcomes and healthcare-associated infection (HAI) metrics.Infect Control Hosp Epidemiol. 2024 Apr;45(4):405-411. doi: 10.1017/ice.2023.284. Epub 2024 Jan 11. Infect Control Hosp Epidemiol. 2024. PMID: 38204365 Free PMC article.
-
Assessment of Federal Value-Based Incentive Programs and In-Hospital Clostridioides difficile Infection Rates.JAMA Netw Open. 2021 Oct 1;4(10):e2132114. doi: 10.1001/jamanetworkopen.2021.32114. JAMA Netw Open. 2021. PMID: 34714336 Free PMC article.
-
Role of diagnostic stewardship in reducing healthcare-facility-onset Clostridioides difficile infections.Antimicrob Steward Healthc Epidemiol. 2023 Mar 16;3(1):e53. doi: 10.1017/ash.2022.305. eCollection 2023. Antimicrob Steward Healthc Epidemiol. 2023. PMID: 36970430 Free PMC article.
-
SHEA/APIC/IDSA/PIDS multisociety position paper: Raising the bar: necessary resources and structure for effective healthcare facility infection prevention and control programs.Infect Control Hosp Epidemiol. 2025 Apr 28;46(7):1-19. doi: 10.1017/ice.2025.73. Online ahead of print. Infect Control Hosp Epidemiol. 2025. PMID: 40289573 Free PMC article.
-
Diagnostic stewardship to limit repeat plasma cytomegalovirus viral load testing.BMC Infect Dis. 2023 Jun 9;23(1):387. doi: 10.1186/s12879-023-08355-0. BMC Infect Dis. 2023. PMID: 37296377 Free PMC article.
