

Birt-Hogg-Dubé syndrome
- PMID: 32943413
- PMCID: PMC9489184
- DOI: 10.1183/16000617.0042-2020
Birt-Hogg-Dubé syndrome
Abstract
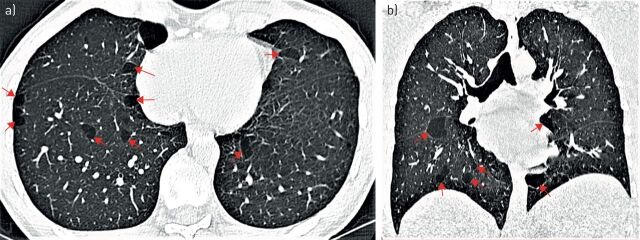
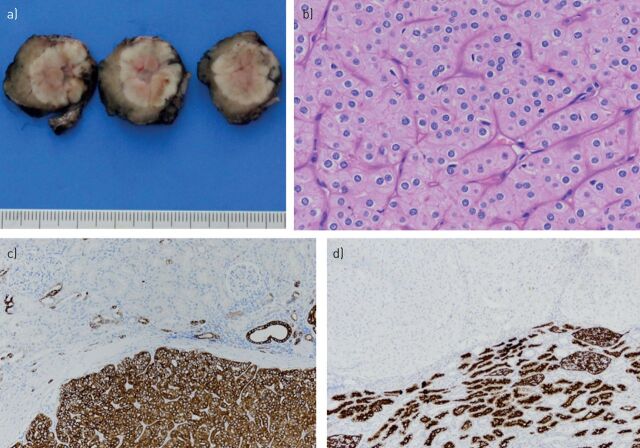
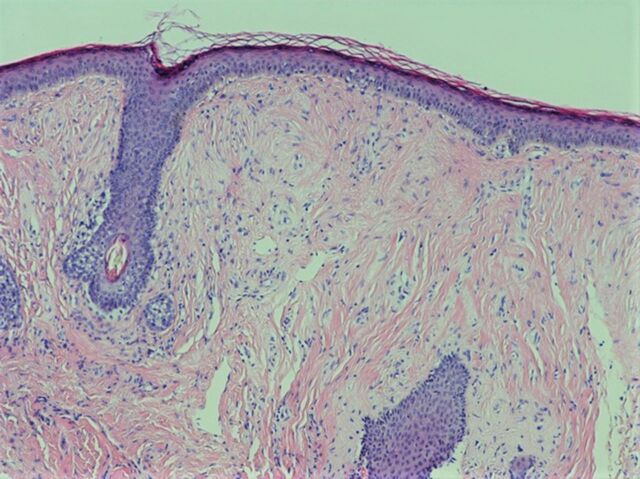
Birt-Hogg-Dubé syndrome (BHD) is a rare inherited autosomal dominant disorder caused by germline mutations in the tumour suppressor gene FLCN, encoding the protein folliculin. Its clinical expression typically includes multiple pulmonary cysts, recurrent spontaneous pneumothoraces, cutaneous fibrofolliculomas and renal tumours of various histological types. BHD has no sex predilection and tends to manifest in the third or fourth decade of life. Multiple bilateral pulmonary cysts are found on chest computed tomography in >80% of patients and more than half experience one or more episodes of pneumothorax. A family history of pneumothorax is an important clue, which suggests the diagnosis of BHD. Unlike other cystic lung diseases such as lymphangioleiomyomatosis and pulmonary Langerhans cell histiocytosis, BHD does not lead to progressive loss of lung function and chronic respiratory insufficiency. Renal tumours affect about 30% of patients during their lifetime, and can be multiple and recurrent. The diagnosis of BHD is based on a combination of genetic, clinical and/or skin histopathological criteria. Management mainly consists of early pleurodesis in the case of pneumothorax, periodic renal imaging for tumour detection, and diagnostic work-up in search of BHD in relatives of the index patient.
Copyright ©ERS 2020.
Conflict of interest statement
Provenance: Commissioned article, peer reviewed. Conflict of interest: C. Daccord reports non-financial support from Boehringer-Ingelheim and Roche, outside the submitted work. Conflict of interest: J-M. Good has nothing to disclose. Conflict of interest: M-A. Morren has nothing to disclose. Conflict of interest: O. Bonny has nothing to disclose. Conflict of interest: D. Hohl has nothing to disclose. Conflict of interest: R. Lazor reports personal fees and non-financial support from Boehringer-Ingelheim, and non-financial support from Roche and Vifor, outside the submitted work.
Figures


Comment in
-
Alveolar proteinosis of genetic origins.Eur Respir Rev. 2020 Oct 28;29(158):190187. doi: 10.1183/16000617.0187-2019. Print 2020 Dec 31. Eur Respir Rev. 2020. PMID: 33115790 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical