

Computerised clinical decision support systems and absolute improvements in care: meta-analysis of controlled clinical trials
- PMID: 32943437
- PMCID: PMC7495041
- DOI: 10.1136/bmj.m3216
Computerised clinical decision support systems and absolute improvements in care: meta-analysis of controlled clinical trials
Abstract
Objective: To report the improvements achieved with clinical decision support systems and examine the heterogeneity from pooling effects across diverse clinical settings and intervention targets.
Design: Systematic review and meta-analysis.
Data sources: Medline up to August 2019.
Eligibility criteria for selecting studies and methods: Randomised or quasi-randomised controlled trials reporting absolute improvements in the percentage of patients receiving care recommended by clinical decision support systems. Multilevel meta-analysis accounted for within study clustering. Meta-regression was used to assess the degree to which the features of clinical decision support systems and study characteristics reduced heterogeneity in effect sizes. Where reported, clinical endpoints were also captured.
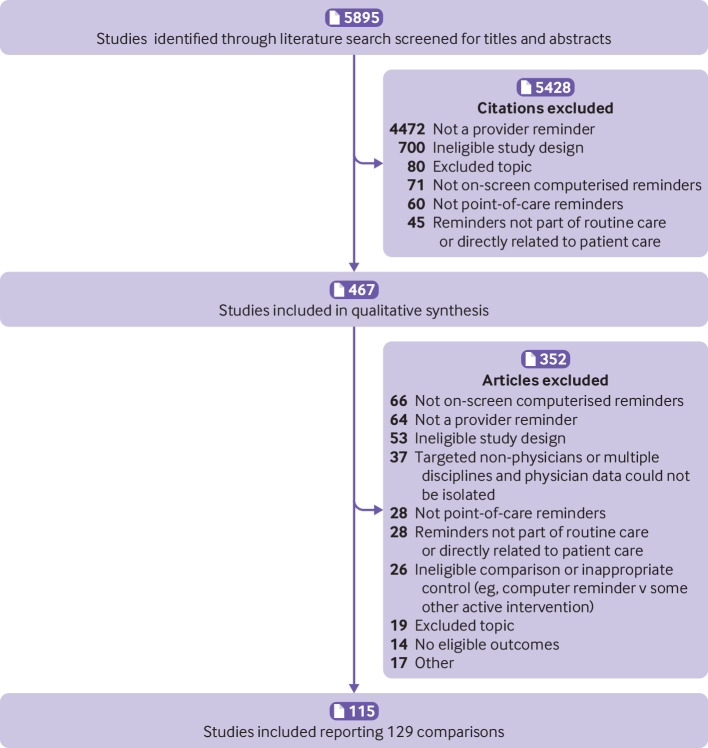
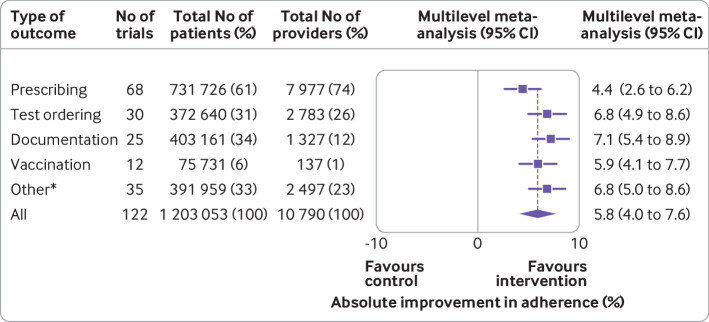
Results: In 108 studies (94 randomised, 14 quasi-randomised), reporting 122 trials that provided analysable data from 1 203 053 patients and 10 790 providers, clinical decision support systems increased the proportion of patients receiving desired care by 5.8% (95% confidence interval 4.0% to 7.6%). This pooled effect exhibited substantial heterogeneity (I2=76%), with the top quartile of reported improvements ranging from 10% to 62%. In 30 trials reporting clinical endpoints, clinical decision support systems increased the proportion of patients achieving guideline based targets (eg, blood pressure or lipid control) by a median of 0.3% (interquartile range -0.7% to 1.9%). Two study characteristics (low baseline adherence and paediatric settings) were associated with significantly larger effects. Inclusion of these covariates in the multivariable meta-regression, however, did not reduce heterogeneity.
Conclusions: Most interventions with clinical decision support systems appear to achieve small to moderate improvements in targeted processes of care, a finding confirmed by the small changes in clinical endpoints found in studies that reported them. A minority of studies achieved substantial increases in the delivery of recommended care, but predictors of these more meaningful improvements remain undefined.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Clinical decision support systems in low resource settings.BMJ. 2020 Oct 14;371:m3962. doi: 10.1136/bmj.m3962. BMJ. 2020. PMID: 33055104 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources