

Systemic complement activation is associated with respiratory failure in COVID-19 hospitalized patients
- PMID: 32943538
- PMCID: PMC7547220
- DOI: 10.1073/pnas.2010540117
Systemic complement activation is associated with respiratory failure in COVID-19 hospitalized patients
Abstract
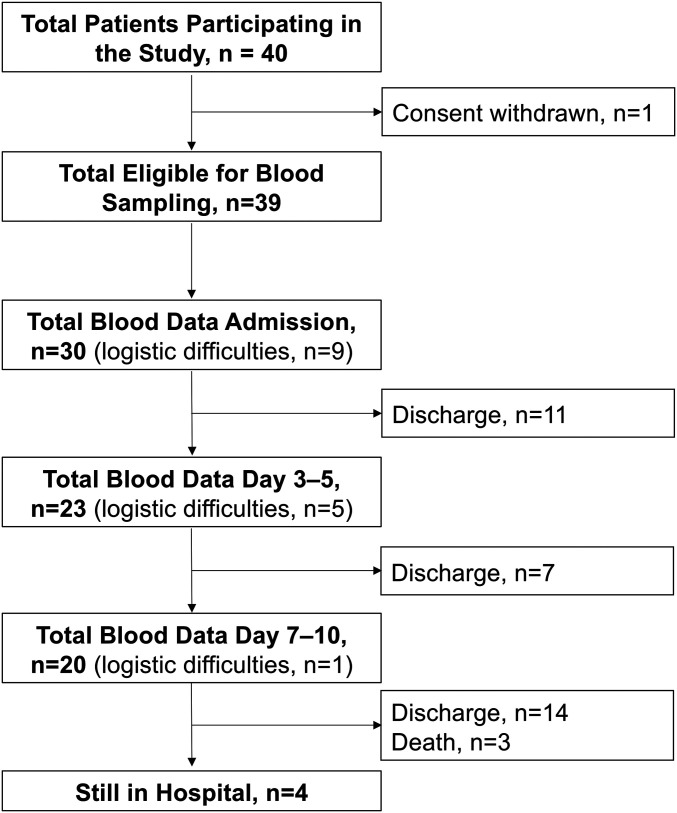
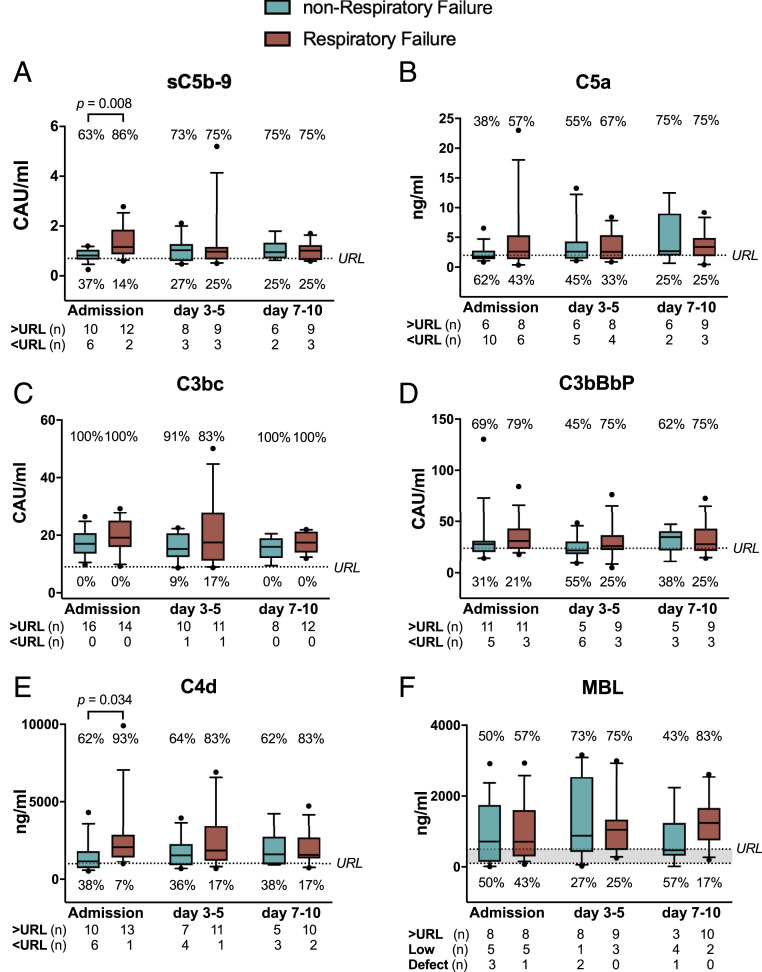
Respiratory failure in the acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic is hypothesized to be driven by an overreacting innate immune response, where the complement system is a key player. In this prospective cohort study of 39 hospitalized coronavirus disease COVID-19 patients, we describe systemic complement activation and its association with development of respiratory failure. Clinical data and biological samples were obtained at admission, days 3 to 5, and days 7 to 10. Respiratory failure was defined as PO2/FiO2 ratio of ≤40 kPa. Complement activation products covering the classical/lectin (C4d), alternative (C3bBbP) and common pathway (C3bc, C5a, and sC5b-9), the lectin pathway recognition molecule MBL, and antibody serology were analyzed by enzyme-immunoassays; viral load by PCR. Controls comprised healthy blood donors. Consistently increased systemic complement activation was observed in the majority of COVID-19 patients during hospital stay. At admission, sC5b-9 and C4d were significantly higher in patients with than without respiratory failure (P = 0.008 and P = 0.034). Logistic regression showed increasing odds of respiratory failure with sC5b-9 (odds ratio 31.9, 95% CI 1.4 to 746, P = 0.03) and need for oxygen therapy with C4d (11.7, 1.1 to 130, P = 0.045). Admission sC5b-9 and C4d correlated significantly to ferritin (r = 0.64, P < 0.001; r = 0.69, P < 0.001). C4d, sC5b-9, and C5a correlated with antiviral antibodies, but not with viral load. Systemic complement activation is associated with respiratory failure in COVID-19 patients and provides a rationale for investigating complement inhibitors in future clinical trials.
Keywords: COVID-19; SARS-CoV-2; complement system; respiratory failure; sC5b-9.
Copyright © 2020 the Author(s). Published by PNAS.
Conflict of interest statement
Competing interest statement: T.E.M. is a member of the Scientific Advisory Board for Ra Pharmaceutical producing complement inhibitors. All other authors declare no competing interests.
Figures
References
-
- Markiewski M. M., Nilsson B., Ekdahl K. N., Mollnes T. E., Lambris J. D., Complement and coagulation: Strangers or partners in crime? Trends Immunol. 28, 184–192 (2007). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
