

SARS-CoV-2 seroprevalence and neutralizing activity in donor and patient blood
- PMID: 32943630
- PMCID: PMC7499171
- DOI: 10.1038/s41467-020-18468-8
SARS-CoV-2 seroprevalence and neutralizing activity in donor and patient blood
Abstract
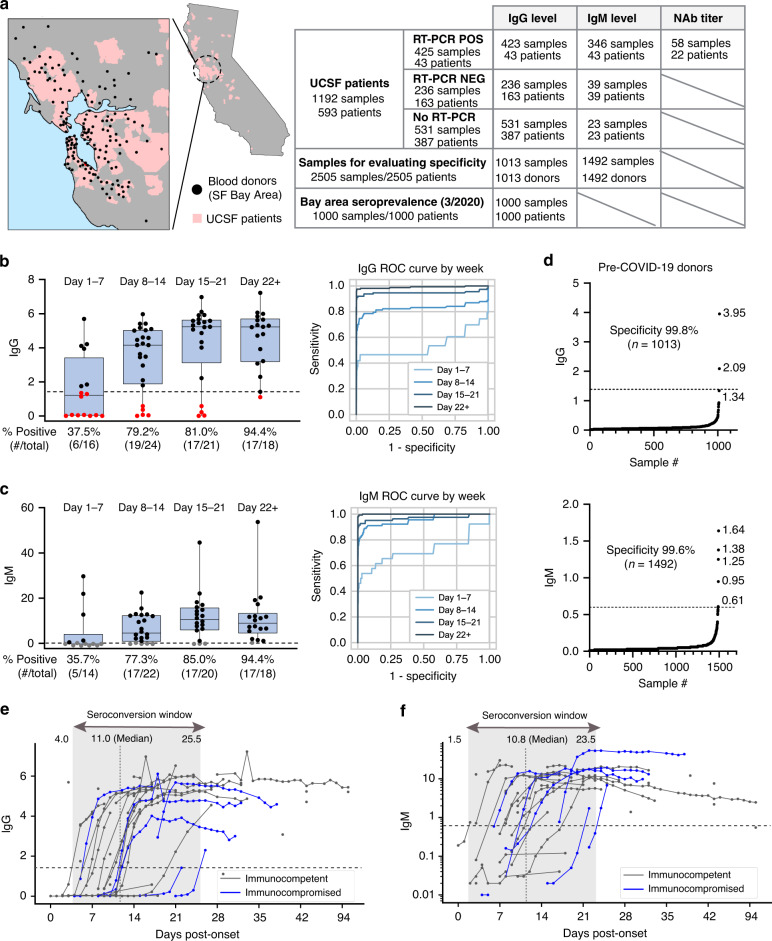
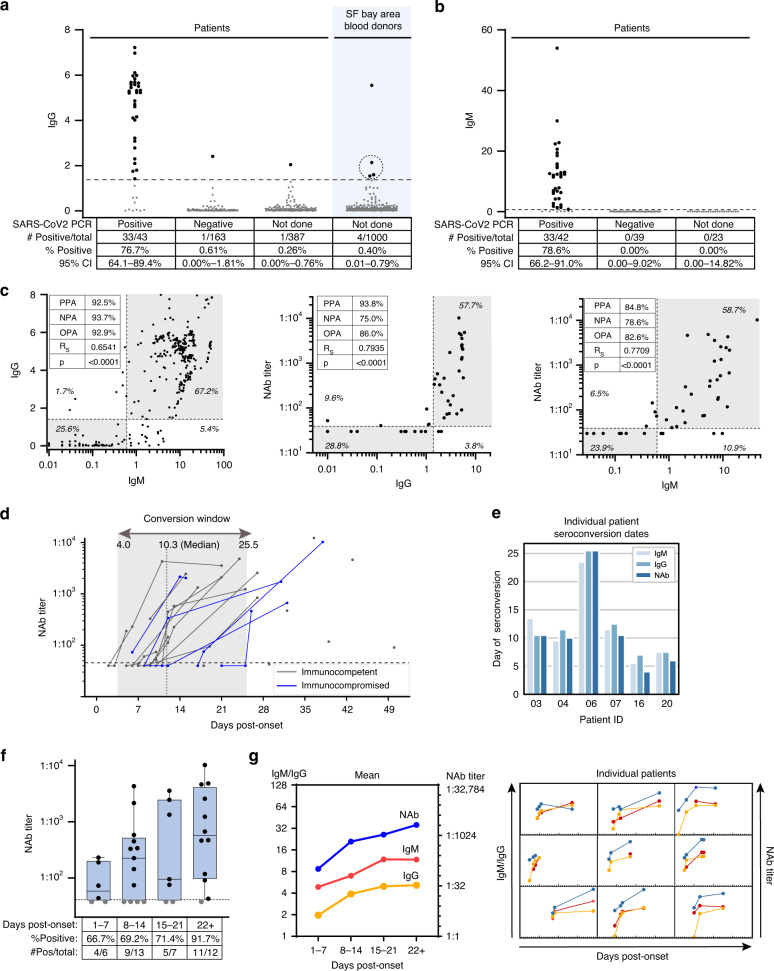
Given the limited availability of serological testing to date, the seroprevalence of SARS-CoV-2-specific antibodies in different populations has remained unclear. Here, we report very low SARS-CoV-2 seroprevalence in two San Francisco Bay Area populations. Seroreactivity was 0.26% in 387 hospitalized patients admitted for non-respiratory indications and 0.1% in 1,000 blood donors in early April 2020. We additionally describe the longitudinal dynamics of immunoglobulin-G (IgG), immunoglobulin-M (IgM), and in vitro neutralizing antibody titers in COVID-19 patients. The median time to seroconversion ranged from 10.3-11.0 days for these 3 assays. Neutralizing antibodies rose in tandem with immunoglobulin titers following symptom onset, and positive percent agreement between detection of IgG and neutralizing titers was >93%. These findings emphasize the importance of using highly accurate tests for surveillance studies in low-prevalence populations, and provide evidence that seroreactivity using SARS-CoV-2 anti-nucleocapsid protein IgG and anti-spike IgM assays are generally predictive of in vitro neutralizing capacity.
Conflict of interest statement
C.Y.C. is the director of the UCSF-Abbott Viral Diagnostics and Discovery Center (VDDC) and receives research support funding from Abbott Laboratories. J.P., M.R., K.C., S.P., and J.R.H., Jr. are employees of Abbott Laboratories. The other authors have no competing interests to declare.
Figures
Update of
-
SARS-CoV-2 seroprevalence and neutralizing activity in donor and patient blood from the San Francisco Bay Area.medRxiv [Preprint]. 2020 May 25:2020.05.19.20107482. doi: 10.1101/2020.05.19.20107482. medRxiv. 2020. Update in: Nat Commun. 2020 Sep 17;11(1):4698. doi: 10.1038/s41467-020-18468-8. PMID: 32511477 Free PMC article. Updated. Preprint.
References
-
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese center for disease control and prevention. J. Am. Med. Assoc. 2020;32:1239–1242. doi: 10.1001/jama.2020.2648. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
