

Pediatric subset of primary immunodeficiency patients treated with SCIG: post hoc analysis of SHIFT and IBIS pooled data
- PMID: 32944034
- PMCID: PMC7491303
- DOI: 10.1186/s13223-020-00478-2
Pediatric subset of primary immunodeficiency patients treated with SCIG: post hoc analysis of SHIFT and IBIS pooled data
Abstract
Background: Primary immunodeficiencies (PID) constitute a heterogeneous group of more than 350 monogenetic diseases. PID patients with antibody impairment require lifelong administration of immunoglobulin G replacement therapy, administered either intravenously (IVIG) or subcutaneously (SCIG). Although the effectiveness of weekly and biweekly (every other week) SCIG administration has been shown in several trials, data on the viability of these two regimens in pediatric PID patients are sparse.
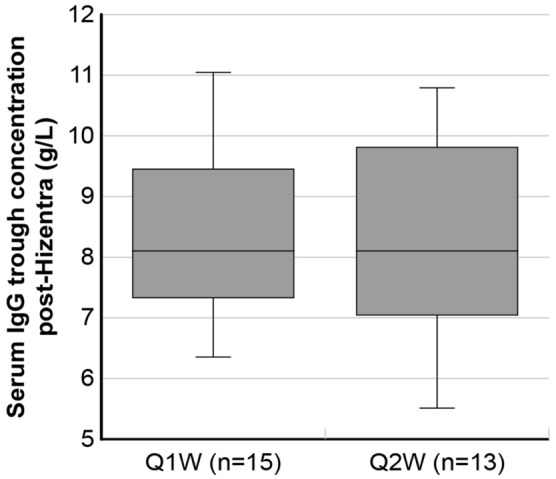
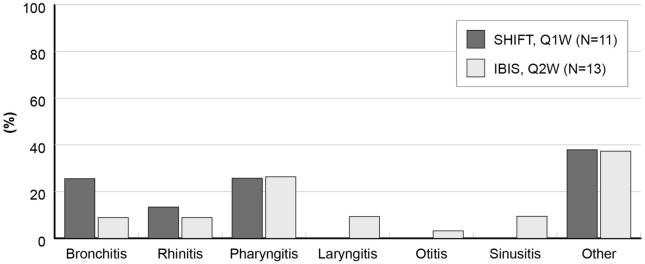
Methods: Data on the pediatric subsets of PID patients enrolled in SHIFT (weekly) and IBIS (biweekly) studies were pooled and analyzed to indirectly compare two different 20%-concentrated SCIG (Hizentra®) regimens. The primary endpoints were to evaluate trough IgG levels and cumulative monthly doses; the secondary endpoint was to analyze incidence of infections.
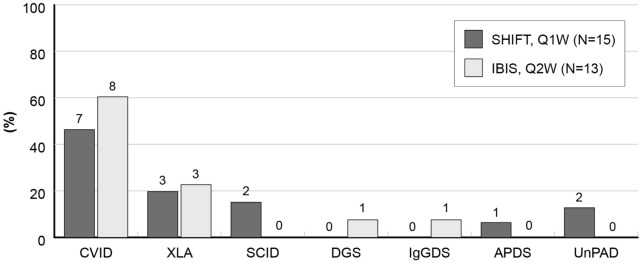
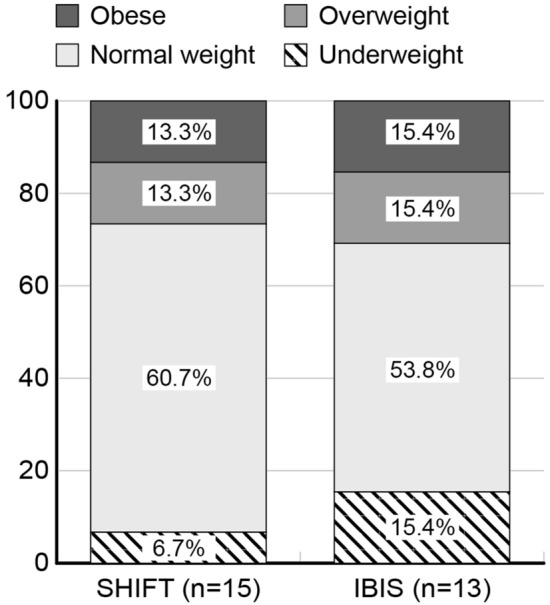
Results: Fifteen and 13 children from the SHIFT and IBIS studies were included, respectively. Cumulative 20%-concentrated SCIG monthly dose was slight lower for the biweekly regimen (Δ = - 2.04, 90% CI - 8.3 to 4.23). However, the trough IgG levels were similar between the two groups (Δ = 0.28, 90% CI - 0.51 to 1.07) and constantly above the threshold of 5 g/L. After adjusting for potential confounders, the annualized rate of infections was similar between SHIFT and IBIS patients (incidence rate ratio = 1.09, 90% CI 0.72-1.67); only 1 serious bacterial infection was experienced by a patient in the IBIS group.
Conclusion: In pediatric PID patients, weekly and biweekly Hizentra® administrations appeared equally effective treatment options.
Keywords: IBIS study; Immunoglobulin; Infection rate; Pediatric patients; Primary immunodeficiency; SHIFT study.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsVM has received honoraria by CSL Behring and has taken part to a board sponsored by Takeda. CC, AT and SG declare that they have no competing interests. BM has received honoraria from Takeda and Kedrion. GMB is an employee of CSL Behring.
Figures
Similar articles
-
Correlations Among Subcutaneous Immunoglobulin Dosage, Immunoglobulin G Serum Pre-infusional Levels and Body Mass Index in Primary Antibody Deficiency Patients: A Pooled Analysis from the SHIFT/IBIS Studies.Clin Drug Investig. 2020 Mar;40(3):279-286. doi: 10.1007/s40261-020-00885-8. Clin Drug Investig. 2020. PMID: 32036588 Free PMC article.
-
Subcutaneous Immunoglobulin Twenty Percent Every Two Weeks in Pediatric Patients with Primary Immunodeficiencies: Subcohort Analysis of the IBIS Study.Pediatr Allergy Immunol Pulmonol. 2019 Jun 1;32(2):70-75. doi: 10.1089/ped.2018.0967. Epub 2019 Jun 17. Pediatr Allergy Immunol Pulmonol. 2019. PMID: 31508259 Free PMC article.
-
Biweekly Hizentra® in Primary Immunodeficiency: a Multicenter, Observational Cohort Study (IBIS).J Clin Immunol. 2018 Jul;38(5):602-609. doi: 10.1007/s10875-018-0528-5. Epub 2018 Jun 28. J Clin Immunol. 2018. PMID: 29951948 Free PMC article.
-
Long-Term Efficacy and Safety of Hizentra® in Patients with Primary Immunodeficiency in Japan, Europe, and the United States: a Review of 7 Phase 3 Trials.J Clin Immunol. 2018 Nov;38(8):864-875. doi: 10.1007/s10875-018-0560-5. Epub 2018 Nov 10. J Clin Immunol. 2018. PMID: 30415311 Free PMC article. Review.
-
Subcutaneous immunoglobulin replacement therapy with Hizentra, the first 20% SCIG preparation: a practical approach.Adv Ther. 2011 Jul;28(7):521-33. doi: 10.1007/s12325-011-0036-y. Epub 2011 Jun 14. Adv Ther. 2011. PMID: 21681653 Review.
References
-
- Food and Drug Administration (FDA). Safety, efficacy, and pharmacokinetic studies to support marketing of immune globulin intravenous (human) as replacement therapy for primary humoral immunodeficiency. Guidance for industry. 2008 https://www.fda.gov/media/124333/download.
-
- Stiehm ER. Human intravenous immunoglobulin in primary and secondary antibody deficiencies. Pediatr Infect Dis J. 1997;16:696–707. - PubMed
-
- Bonagura VR, Marchlewski R, Cox A, Rosenthal DW. Biologic IgG level in primary immunodeficiency disease: the IgG level that protects against recurrent infection. J Allergy Clin Immunol. 2008 - PubMed
-
- Chapel HM, Spickett GP, Ericson D, Engl W, Eibl MM, Bjorkander J. The comparison of the efficacy and safety of intravenous versus subcutaneous immunoglobulin replacement therapy. J Clin Immunol. 2000;20:94–100. - PubMed
LinkOut - more resources
Full Text Sources
