

Experimental artefacts can lead to misattribution of bioactivity from soluble mesenchymal stem cell paracrine factors to extracellular vesicles
- PMID: 32944192
- PMCID: PMC7480412
- DOI: 10.1080/20013078.2020.1807674
Experimental artefacts can lead to misattribution of bioactivity from soluble mesenchymal stem cell paracrine factors to extracellular vesicles
Abstract
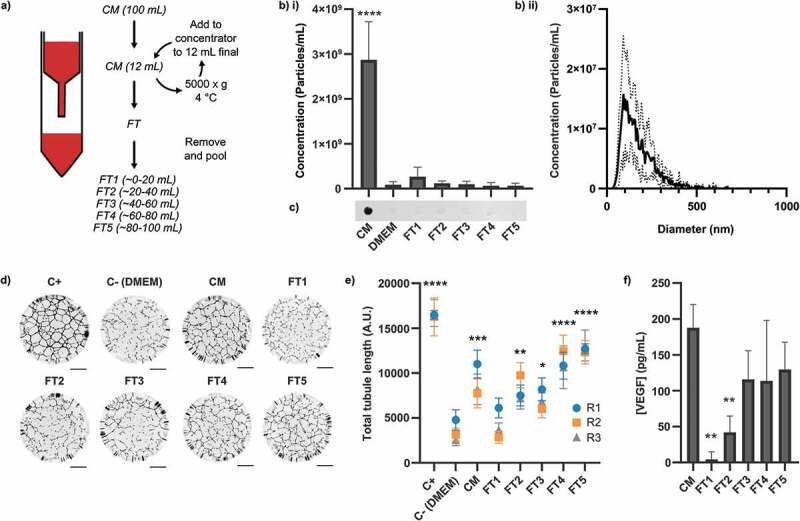
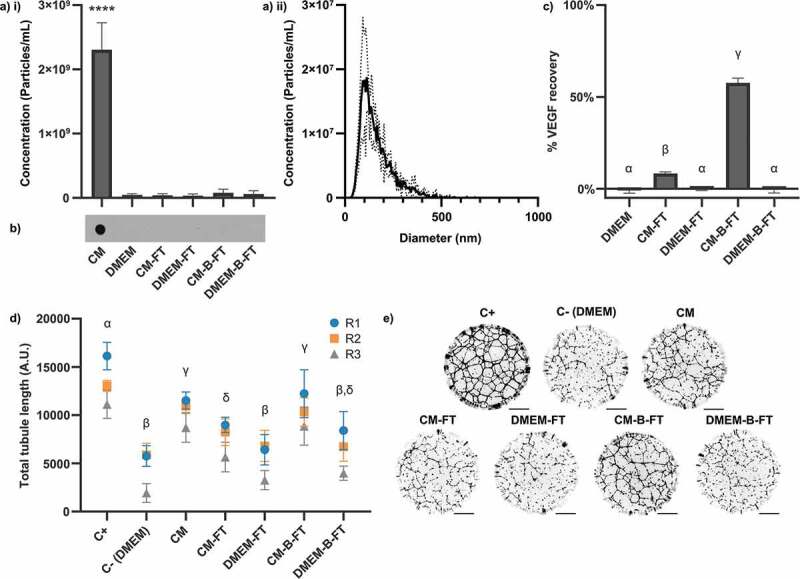
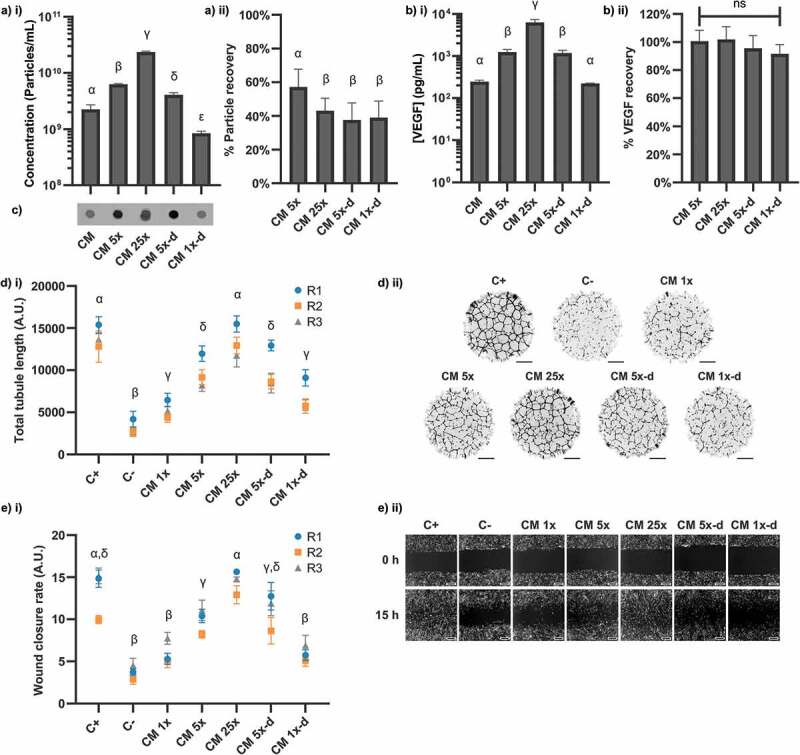
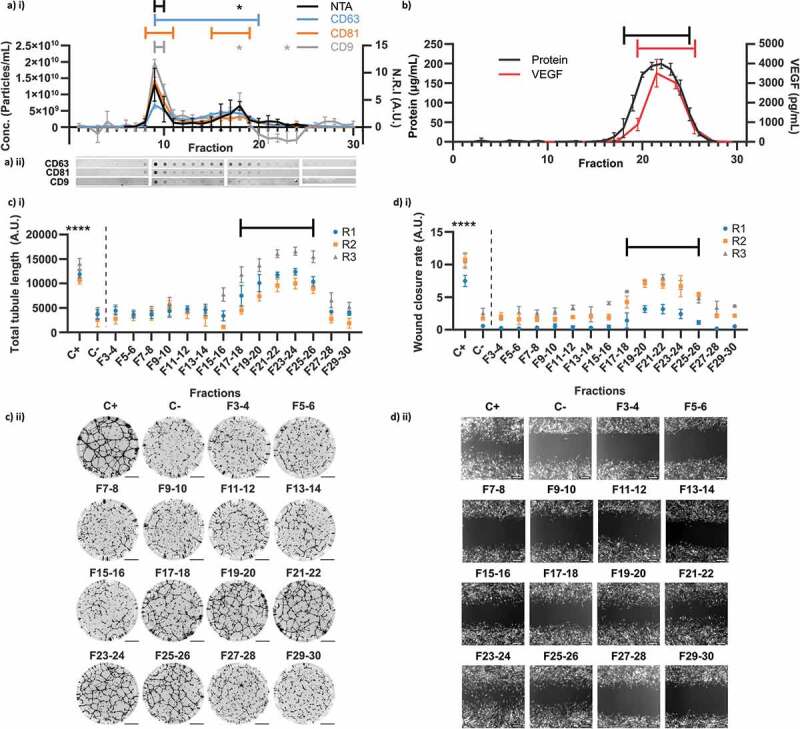
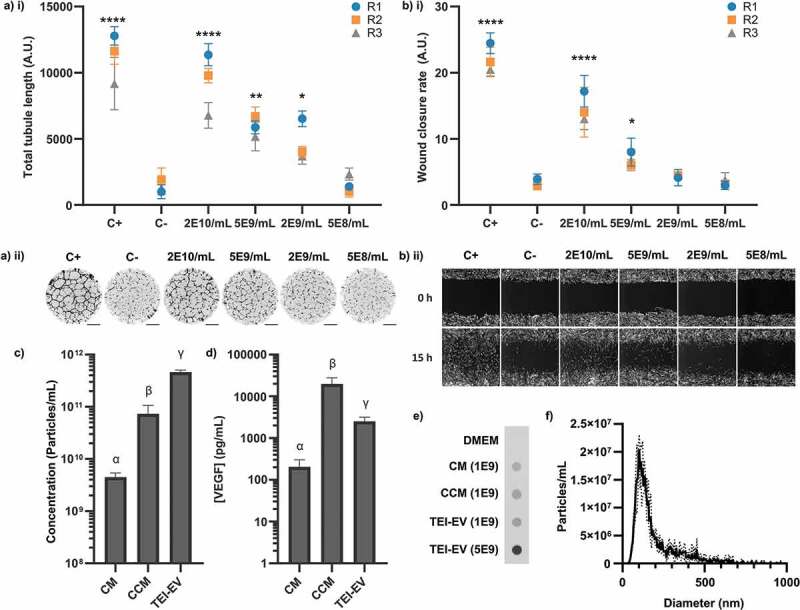
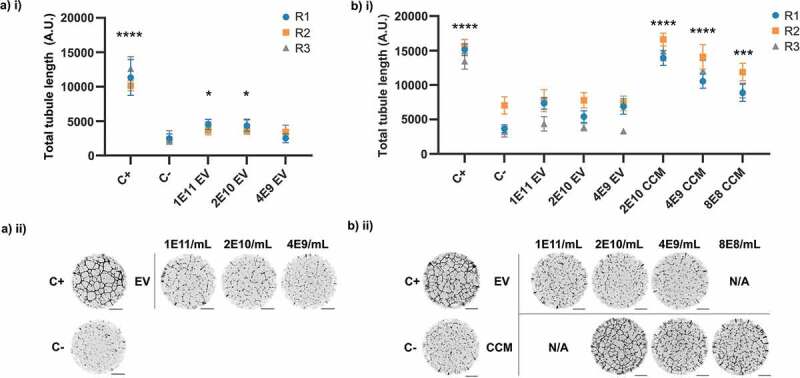
It has been demonstrated that some commonly used Extracellular Vesicle (EV) isolation techniques can lead to substantial contamination with non-EV factors. Whilst it has been established that this impacts the identification of biomarkers, the impact on apparent EV bioactivity has not been explored. Extracellular vesicles have been implicated as critical mediators of therapeutic human mesenchymal stem cell (hMSC) paracrine signalling. Isolated hMSC-EVs have been used to treat multiple in vitro and in vivo models of tissue damage. However, the relative contributions of EVs and non-EV factors have not been directly compared. The dependence of hMSC paracrine signalling on EVs was first established by ultrafiltration of hMSC-conditioned medium to deplete EVs, which led to a loss of signalling activity. Here, we show that this method also causes depletion of non-EV factors, and that when this is prevented proangiogenic signalling activity is fully restored in vitro. Subsequently, we used size-exclusion chromatography (SEC) to separate EVs and soluble proteins to directly and quantitatively compare their relative contributions to signalling. Non-EV factors were found to be necessary and sufficient for the stimulation of angiogenesis and wound healing in vitro. EVs in isolation were found to be capable of potentiating signalling only when isolated by a low-purity method, or when used at comparatively high concentrations. These results indicate a potential for contaminating soluble factors to artefactually increase the apparent bioactivity of EV isolates and could have implications for future studies on the biological roles of EVs.
Keywords: Extracellular vesicles; angiogenesis; contamination; exosomes; mesenchymal stem cell; microvesicles; paracrine effect; polymer precipitation; purification; size exclusion.
© 2020 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group on behalf of The International Society for Extracellular Vesicles.
Conflict of interest statement
No funding agency was involved in the study design, data collection, data management, analysis, interpretation or preparation of the manuscript. No conflicts of interest are declared.
Figures
References
-
- Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2018;39(42):3757–3758. - PubMed
-
- Hopkins C, Li J, Rae F, et al. Stem cell options for kidney disease. J Pathol. 2009;217(2):265–281. - PubMed
-
- Morigi M. Mesenchymal stem cells are renotropic, helping to repair the kidney and improve function in acute renal failure. J Am Soc Nephrol. 2004;15(7):1794–1804. - PubMed
-
- Choi YH, Kurtz A, Stamm C. Mesenchymal stem cells for cardiac cell therapy. Hum Gene Ther. 2011;22(1):3–17. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
