

Evaluation of ultrasound-guided erector spinae plane block for postoperative management of video-assisted thoracoscopic surgery: a prospective, randomized, controlled clinical trial
- PMID: 32944329
- PMCID: PMC7475548
- DOI: 10.21037/jtd-20-689
Evaluation of ultrasound-guided erector spinae plane block for postoperative management of video-assisted thoracoscopic surgery: a prospective, randomized, controlled clinical trial
Abstract
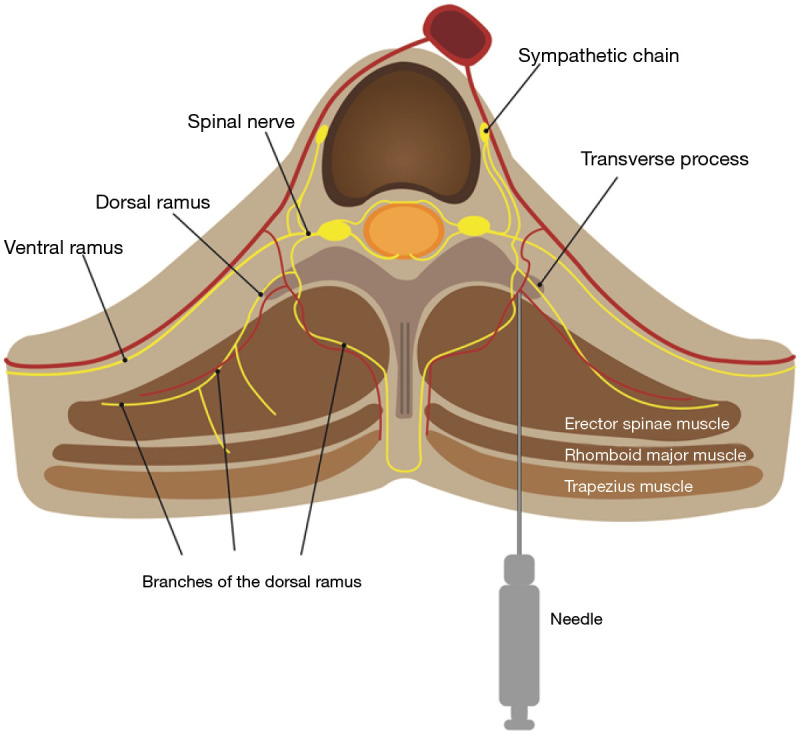
Background: Video-assisted thoracoscopic surgery (VATS) is a commonly performed minimally invasive procedure that has led to lower levels of pain, as well as procedure-related mortality and morbidity. However, VATS requires analgesia that blocks both visceral and somatic nerve fibers for more effective pain control. This randomized controlled trial evaluated the effect of erector spinae plane block (ESPB) in the postoperative analgesia management of patients undergoing VATS.
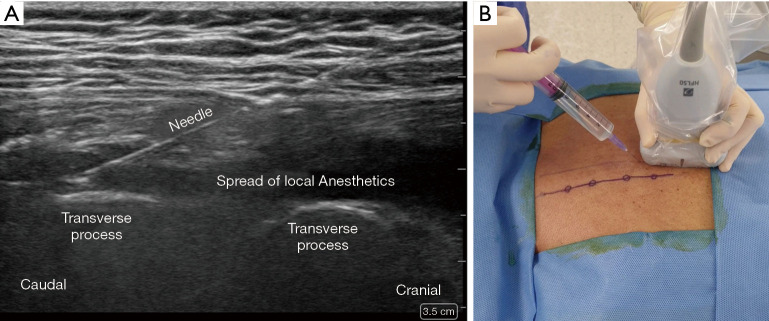
Methods: We performed a prospective, randomized, single-center study between December 2018 and December 2019. Fifty-four patients were recruited to two equal groups (ESPB and control group). Following exclusion, 46 patients were included in the final analysis. Patients were randomly assigned to receive preoperative ultrasound-guided ESPB with either ropivacaine or saline. The primary outcome was the numeric rating scale (NRS) score, assessed 12 hours postoperatively. Secondary outcomes were the Riker Sedation-Agitation Scale (SAS) score for emergence agitation, postoperative cumulative opioid consumption, length of post-anesthesia care unit (PACU) stay, incidence of postoperative nausea and vomiting (PONV) and dizziness, and ESPB-related adverse events.
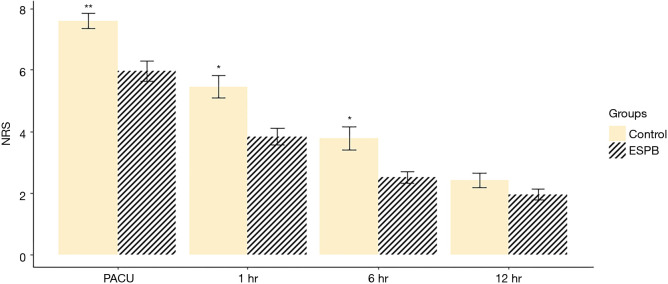
Results: The NRS in the ESPB group during the postoperative period immediately after PACU admission was significantly lower than that in the control group (5.96±1.68 and 7.59±1.18, respectively; P<0.001) and remained lower until 6 hours postoperatively (P=0.001 at 1 hour and P=0.005 at 6 hours). At 12 hours postoperatively, NRS scores were not significantly different between groups (P=0.12). The median [interquartile range (IQR)] of the postoperative rescue pethidine consumption in PACU was significantly lower [25 mg (25 mg)] in the ESPB group than that in the control group [50 mg (56.2 mg); P=0.006]. The median (IQR) of PACU residual time was significantly lower [25 min (10 min)] in the ESPB group than that in the control group [30 min (15 min); P=0.034]. The median (IQR) Riker SAS was also lower in the ESPB group [4 (1.0)] than that in the control group [5 (1.25); P<0.001] in PACU.
Conclusions: A single preoperative injection of ESPB with ropivacaine may improve acute postoperative analgesia and emergence agitation in patients undergoing VATS.
Keywords: Video-assisted thoracoscopic surgery (VATS); erector spinae plane block; paravertebral block; thoracic epidural blockade; ultrasound.
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/jtd-20-689). The authors have no conflicts of interest to declare.
Figures

References
-
- Falcoz PE, Puyraveau M, Thomas PA, et al. Video-assisted thoracoscopic surgery versus open lobectomy for primary non-small-cell lung cancer: a propensity-matched analysis of outcome from the European Society of Thoracic Surgeon database. Eur J Cardiothorac Surg 2016;49:602-9. 10.1093/ejcts/ezv154 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical