

Epidemiology, bacteriology, and clinical characteristics of HACEK bacteremia and endocarditis: a population-based retrospective study
- PMID: 32944895
- PMCID: PMC7892745
- DOI: 10.1007/s10096-020-04035-y
Epidemiology, bacteriology, and clinical characteristics of HACEK bacteremia and endocarditis: a population-based retrospective study
Abstract
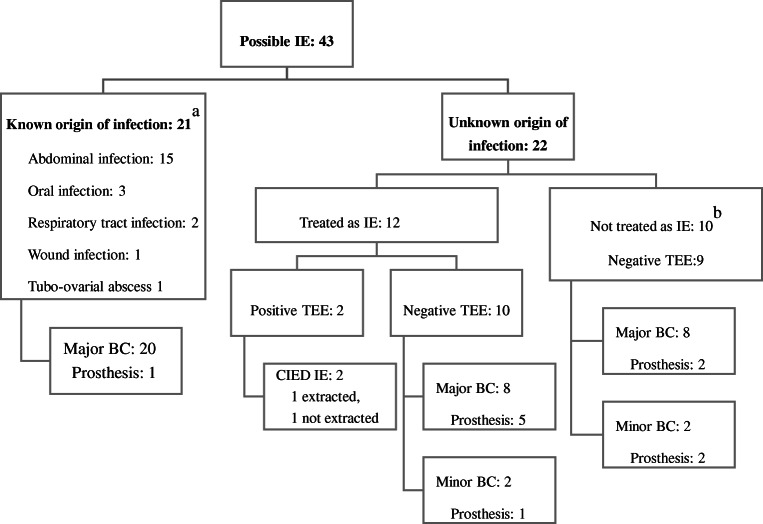
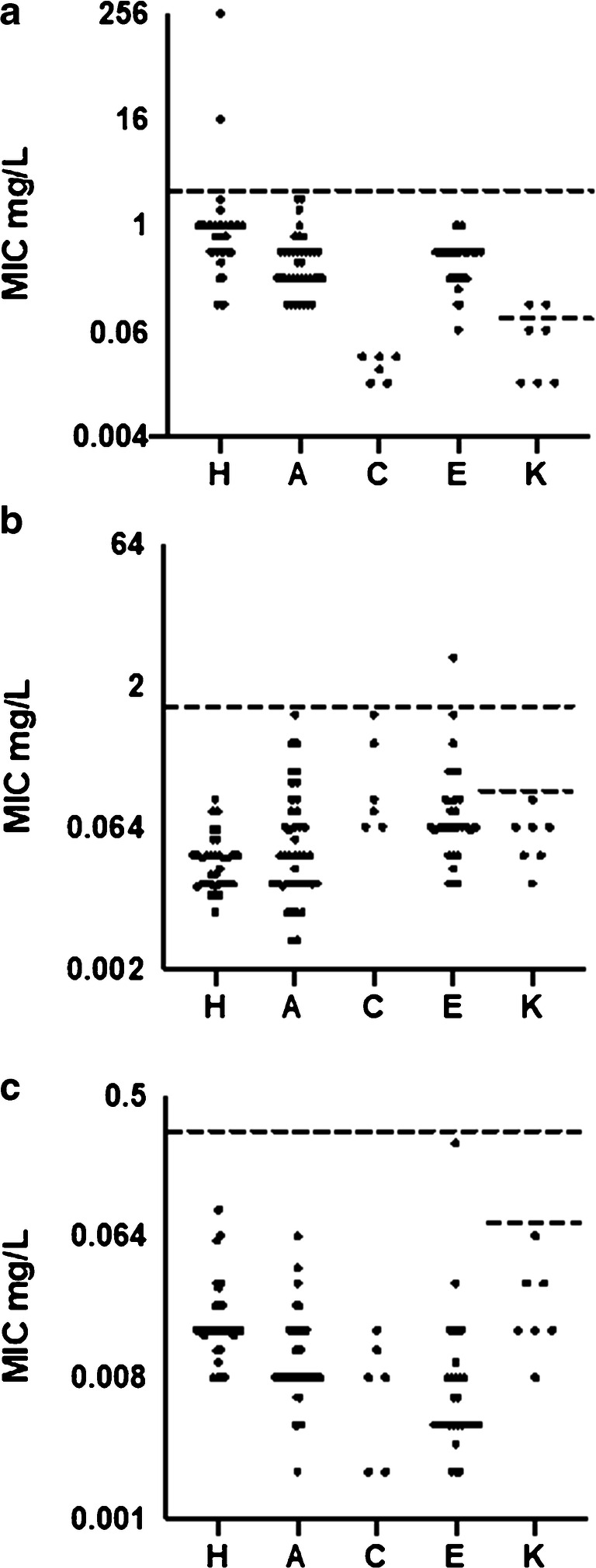
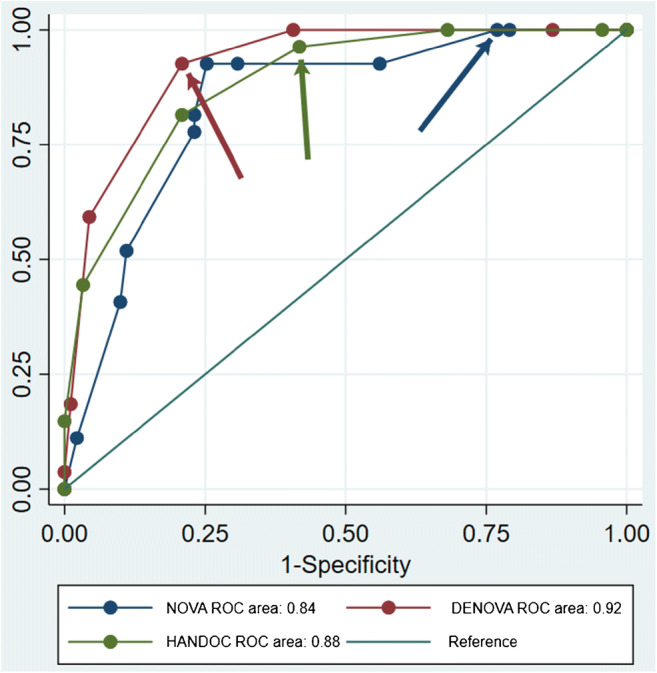
The objective was to describe the epidemiology, bacteriology, clinical presentation, risk factors for endocarditis (IE), diagnostic workup, and outcome of patients with bacteremia caused by the non-influenzae Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, and Kingella genera (HACEK). A retrospective population-based cohort of patients with bacteremia collected from 2012 to 2017 was identified. Clinical data from identified patients were collected from medical records to classify patients, calculate incidences, analyze risk factors of IE, and describe the management and outcome of the cohort. A total of 118 episodes of HACEK bacteremia were identified, of which 27 were definite IE. The incidence of HACEK bacteremia was 5.2 and of HACEK IE 1.2 episodes per 1,000,000 inhabitants per year. Other focal infections were identified in 55 of 118 of the episodes, most commonly within the abdomen (26 episodes). The propensity to cause IE ranged from 62 in Aggregatibacter actinomycetemcomitans to 6% in Eikenella. Risk factors for IE were cardiac implantable electronical device, predisposing cardiac conditions, community acquisition, long duration of symptoms, multiple positive blood cultures, fever, heart murmur, embolization, and unknown origin of infection. The scoring system DENOVA developed to predict IE in bacteremia with Enterococcus faecalis also had a high sensitivity and specificity for predicting IE in HACEK bacteremia. The 30-day mortality was 4% in IE and 15% in non-IE bacteremia, and only one case of relapse was found. IE is common in bacteremia with Aggregatibacter, Cardiobacterium, and Kingella but relatively rare in Haemophilus and Eikenella. Treatment failures are very rare, and DENOVA can be used to evaluate the need for transesophageal echocardiography.
Keywords: Bacteremia; Echocardiography; Endocarditis; Epidemiology; HACEK; Management score.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, Dulgheru R, El Khoury G, Erba PA, Iung B, Miro JM, Mulder BJ, Plonska-Gosciniak E, Price S, Roos-Hesselink J, Snygg-Martin U, Thuny F, Tornos Mas P, Vilacosta I, Zamorano JL, Group ESCSD 2015 ESC guidelines for the management of infective endocarditis: the task force for the management of infective endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM) Eur Heart J. 2015;36(44):3075–3128. doi: 10.1093/eurheartj/ehv319. - DOI - PubMed
-
- Bouza E, Kestler M, Beca T, Mariscal G, Rodriguez-Creixems M, Bermejo J, Fernandez-Cruz A, Fernandez-Aviles F, Munoz P. The NOVA score: a proposal to reduce the need for transesophageal echocardiography in patients with enterococcal bacteremia. Clin Infect Dis. 2015;60(4):528–535. doi: 10.1093/cid/ciu872. - DOI - PubMed
-
- Palraj BR, Baddour LM, Hess EP, Steckelberg JM, Wilson WR, Lahr BD, Sohail MR. Predicting risk of endocarditis using a clinical tool (PREDICT): scoring system to guide use of echocardiography in the management of Staphylococcus aureus bacteremia. Clin Infect Dis. 2015;61(1):18–28. doi: 10.1093/cid/civ235. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
