

Imaging of children with COVID-19: experience from a tertiary children's hospital in the United States
- PMID: 32945888
- PMCID: PMC7498743
- DOI: 10.1007/s00247-020-04830-x
Imaging of children with COVID-19: experience from a tertiary children's hospital in the United States
Abstract
Background: Imaging of novel coronavirus disease 2019 (COVID-19) has been described in adults, but children have milder forms of disease. Pediatric imaging descriptions are of asymptomatic children, raising the question of whether imaging is needed in this patient group.
Objective: To describe the utilization and imaging findings in children with COVID-19 along with the comorbidities, treatment and short-term outcomes.
Materials and methods: We retrospectively reviewed pediatric patients who had a confirmed positive test for COVID-19 during a 2-month period. We noted symptoms and presence of imaging at presentation. Comorbidities were recorded for children with imaging. Children were categorized as having multisystem inflammatory syndrome in children (MIS-C) if they met criteria for the disorder. For children who were admitted to the hospital, we documented length of hospital stay, need for intensive care unit care/ventilator support, and treatment regimen. We evaluated all imaging for acute/chronic abnormalities including chest radiographs for interstitial or alveolar opacities, distribution/symmetry of disease, zonal predominance, and pleural abnormalities. We performed descriptive statistics and compared children with MIS-C with the cohort using a Fisher exact test.
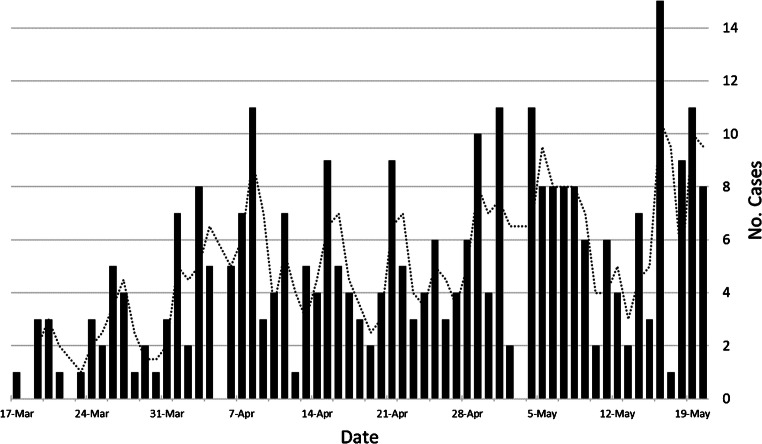
Results: During the study period, 5,969 children were tested for COVID-19, with 313 (5%) testing positive. Of these, 92/313 (29%) were asymptomatic and 55/313 (18%) had imaging and were admitted to the hospital for treatment. Forty-one of 55 patients (75%) with imaging had comorbidities. Chest radiographs were the most common examination (51/55 patients, or 93%) with most demonstrating no abnormality (34/51, or 67%). Children with MIS-C were more likely to have interstitial opacities and pleural effusions. US, CT or MRI was performed in 23/55 (42%) children, 9 of whom had MIS-C. Only one chest CT was performed.
Conclusion: In our study, most pediatric patients with COVID-19 did not require hospital admission or imaging. Most children with imaging had comorbidities but children with MIS-C were more likely to have no comorbidities. Children with imaging mostly had normal chest radiography. Advanced imaging (US, CT, MRI) was less common for the care of these children, particularly CT examination of the chest and for children without MIS-C.
Keywords: COVID-19; Chest; Children; Computed tomography; Coronavirus; Multisystem inflammatory syndrome in children; Radiography; Utilization.
Conflict of interest statement
None
Figures
Similar articles
-
Chest radiograph features of multisystem inflammatory syndrome in children (MIS-C) compared to pediatric COVID-19.Pediatr Radiol. 2021 Feb;51(2):231-238. doi: 10.1007/s00247-020-04921-9. Epub 2021 Jan 6. Pediatr Radiol. 2021. PMID: 33404786 Free PMC article.
-
Imaging Findings in Multisystem Inflammatory Syndrome in Children (MIS-C) Associated With Coronavirus Disease (COVID-19).AJR Am J Roentgenol. 2021 Feb;216(2):507-517. doi: 10.2214/AJR.20.24032. Epub 2020 Jul 29. AJR Am J Roentgenol. 2021. PMID: 32755212
-
COVID-19 in pediatric patients: a case series from the Bronx, NY.Pediatr Radiol. 2020 Sep;50(10):1369-1374. doi: 10.1007/s00247-020-04782-2. Epub 2020 Jul 29. Pediatr Radiol. 2020. PMID: 32728901 Free PMC article.
-
Human and novel coronavirus infections in children: a review.Paediatr Int Child Health. 2021 Feb;41(1):36-55. doi: 10.1080/20469047.2020.1781356. Epub 2020 Jun 25. Paediatr Int Child Health. 2021. PMID: 32584199 Review.
-
Imaging findings in acute pediatric coronavirus disease 2019 (COVID-19) pneumonia and multisystem inflammatory syndrome in children (MIS-C).Pediatr Radiol. 2022 Sep;52(10):1985-1997. doi: 10.1007/s00247-022-05393-9. Epub 2022 May 26. Pediatr Radiol. 2022. PMID: 35616701 Free PMC article. Review.
Cited by
-
Pediatric Radiology in Era of COVID-19, International Consensus and What Lies Beyond Pneumonia: A Review.JNMA J Nepal Med Assoc. 2021 Nov 15;59(243):1196-1203. doi: 10.31729/jnma.7122. JNMA J Nepal Med Assoc. 2021. PMID: 35199747 Free PMC article. Review.
-
Factors Associated with the Antibiotic Treatment of Children Hospitalized for COVID-19 during the Lockdown in Serbia.Int J Environ Res Public Health. 2022 Nov 24;19(23):15590. doi: 10.3390/ijerph192315590. Int J Environ Res Public Health. 2022. PMID: 36497665 Free PMC article.
-
Computed tomography findings in 3,557 COVID-19 infected children: a systematic review.Quant Imaging Med Surg. 2021 Nov;11(11):4644-4660. doi: 10.21037/qims-20-1410. Quant Imaging Med Surg. 2021. PMID: 34737930 Free PMC article. Review.
-
Pulmonary imaging in coronavirus disease 2019 (COVID-19): a series of 140 Latin American children.Pediatr Radiol. 2021 Aug;51(9):1597-1607. doi: 10.1007/s00247-021-05055-2. Epub 2021 Apr 1. Pediatr Radiol. 2021. PMID: 33791841 Free PMC article.
-
Epidemiology and clinical features of SARS-CoV-2 infection in children and adolescents in the pre-Omicron era: A global systematic review and meta-analysis.J Glob Health. 2024 Mar 1;14:05003. doi: 10.7189/jogh.14.05003. J Glob Health. 2024. PMID: 38419461 Free PMC article.
References
-
- Paraluppi V, Pintus MC, Fanos V, Marcialis A. COVID-19 in newborns and in children: the state of the art. J Pediatr Neonatal Individ Med. 2020;9:1–13.
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
