

Evaluation of the interrater and intermethod agreement of the German multiparametric ultrasound criteria for the grading of internal carotid artery stenosis
- PMID: 32945912
- PMCID: PMC7966642
- DOI: 10.1007/s00234-020-02546-1
Evaluation of the interrater and intermethod agreement of the German multiparametric ultrasound criteria for the grading of internal carotid artery stenosis
Abstract
Purpose: The interdisciplinary German guidelines for the diagnosis and treatment of internal carotid artery stenosis (ICAS) recommend a multiparametric approach for the sonographic grading of extracranial ICAS. The aim of this study is to evaluate the interrater and intermethod agreement of this elaborated sonographic approach with different angiographic modalities.
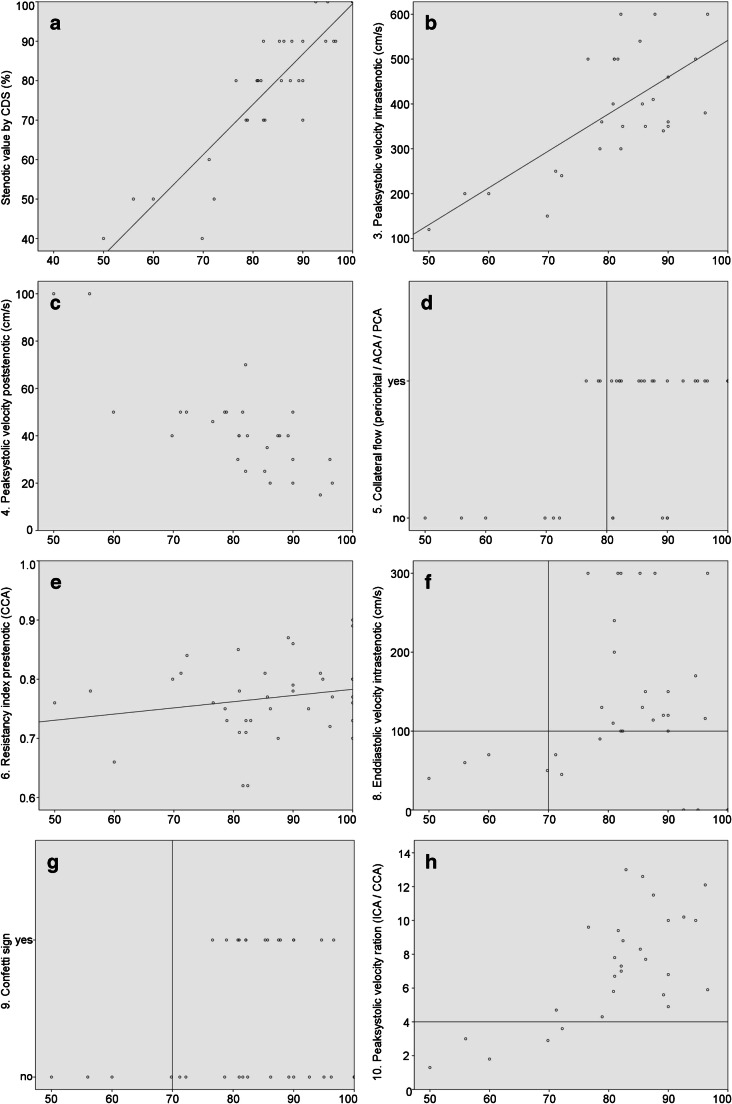
Methods: Patients with extracranial ICAS were examined twice with colour-coded duplex sonography (CDS) by two experienced vascular neurologists. Each of the ten criteria and the resulting stenotic value were assessed. Grading of ICAS based on the multiparametric ultrasound criteria was compared with different angiography modalities (magnetic resonance angiography (MRA), computed tomography angiography (CTA), digital subtraction angiography (DSA)).
Results: Seventy-four consecutive patients with 91 extracranial ICAS were recruited from our stroke unit and neurovascular outpatient clinic. Interrater agreement for each single ultrasound criterion ranged from moderate to excellent (for the peak systolic velocity). Concerning the absolute stenotic value of ICAS, an excellent agreement between both ultrasound examiners with an ICC of 0.91 (range 0.87-0.94; p < 0.001) was found. In 96% of ICAS, the difference between the stenotic values was ≤ 10%. Intermethod agreements between CDS and DSA, CTA, and MRA were also good for both sonographers.
Conclusion: Strictly adhering to the multiparametric "DEGUM ultrasound criteria", we found an excellent interrater agreement and a good intermethod agreement compared with angiography for the sonographic grading of extracranial ICAS. Thus, multiparametric CDS is in particular suitable for the follow up of extracranial ICAS even when examinations are done by different sonographers.
Keywords: Carotid artery disease; DEGUM ultrasound criteria; Grading of internal carotid artery stenosis; Interrater and intermethod agreement; Ultrasound.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


Similar articles
-
Multiparametric 3D Contrast-Enhanced Ultrasound to Assess Internal Carotid Artery Stenosis: A Pilot Study.J Neuroimaging. 2020 Jan;30(1):82-89. doi: 10.1111/jon.12662. Epub 2019 Sep 9. J Neuroimaging. 2020. PMID: 31498524
-
Quantification of Internal Carotid Artery Stenosis with 3D Ultrasound Angiography.Ultraschall Med. 2015 Oct;36(5):487-93. doi: 10.1055/s-0034-1398749. Epub 2015 Jan 21. Ultraschall Med. 2015. PMID: 25607630
-
Evaluation of Freehand B-Mode and Power-Mode 3D Ultrasound for Visualisation and Grading of Internal Carotid Artery Stenosis.PLoS One. 2017 Jan 3;12(1):e0167500. doi: 10.1371/journal.pone.0167500. eCollection 2017. PLoS One. 2017. PMID: 28045903 Free PMC article.
-
False-negative magnetic resonance angiography with extracranial internal carotid artery stenosis: a report of two cases and review of the literature.Neurosurg Rev. 2005 Apr;28(2):154-8. doi: 10.1007/s10143-004-0354-5. Epub 2004 Oct 8. Neurosurg Rev. 2005. PMID: 15480890 Review.
-
[Revision of DEGUM ultrasound criteria for grading internal carotid artery stenoses and transfer to NASCET measurement].Ultraschall Med. 2010 Jun;31(3):251-7. doi: 10.1055/s-0029-1245336. Epub 2010 Apr 22. Ultraschall Med. 2010. PMID: 20414854 Review. German.
Cited by
-
Validity of Ultrasound for the Diagnosis of Arterial Thoracic Outlet Syndrome.EJVES Vasc Forum. 2024 Feb 14;61:92-98. doi: 10.1016/j.ejvsvf.2024.02.003. eCollection 2024. EJVES Vasc Forum. 2024. PMID: 38455254 Free PMC article.
-
Validity and Reliability of Point-of-Care Ultrasound for Detecting Moderate- or High-Grade Carotid Atherosclerosis in an Outpatient Department.Diagnostics (Basel). 2023 Jun 2;13(11):1952. doi: 10.3390/diagnostics13111952. Diagnostics (Basel). 2023. PMID: 37296805 Free PMC article.
References
-
- S3-Leitlinie zur Diagnostik, Therapie und Nachsorge der extracraniellen Carotisstenose. AWMF-Registernummer: 004-028. https://www.awmf.org/uploads/tx_szleitlinien/004-028l_extracranielle-Car.... Accessed 14.05.2020.
MeSH terms
LinkOut - more resources
Full Text Sources
