

Cause-Specific Mortality Following Initial Chemotherapy in a Population-Based Cohort of Patients With Classical Hodgkin Lymphoma, 2000-2016
- PMID: 32946352
- PMCID: PMC7723686
- DOI: 10.1200/JCO.20.00264
Cause-Specific Mortality Following Initial Chemotherapy in a Population-Based Cohort of Patients With Classical Hodgkin Lymphoma, 2000-2016
Abstract
Purpose: Mortality for patients with classical Hodgkin lymphoma (cHL) treated during an era characterized in the United States by widespread use of doxorubicin, bleomycin, vinblastine, and dacarbazine and diminishing use of radiotherapy is not well understood.
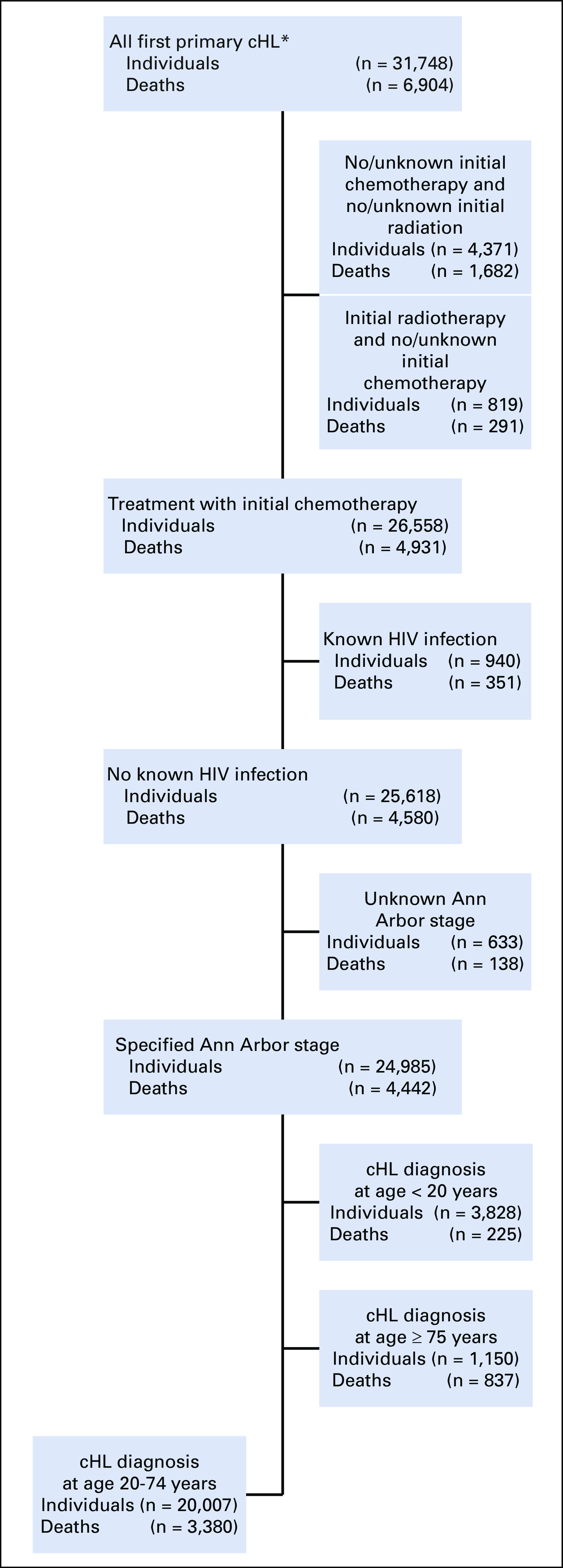
Patients and methods: We identified 20,007 individuals diagnosed with stage I/II (early) or III/IV (advanced) cHL between age 20 and 74 years treated with initial chemotherapy in US population-based cancer registries during 2000-2015 (follow-up through 2016). We used standardized mortality ratios (SMRs) to compare cause-specific relative mortality risk following cHL to that expected in the general population and estimated excess absolute risks (EARs; per 10,000 patient-years) to quantify disease-specific death burden.
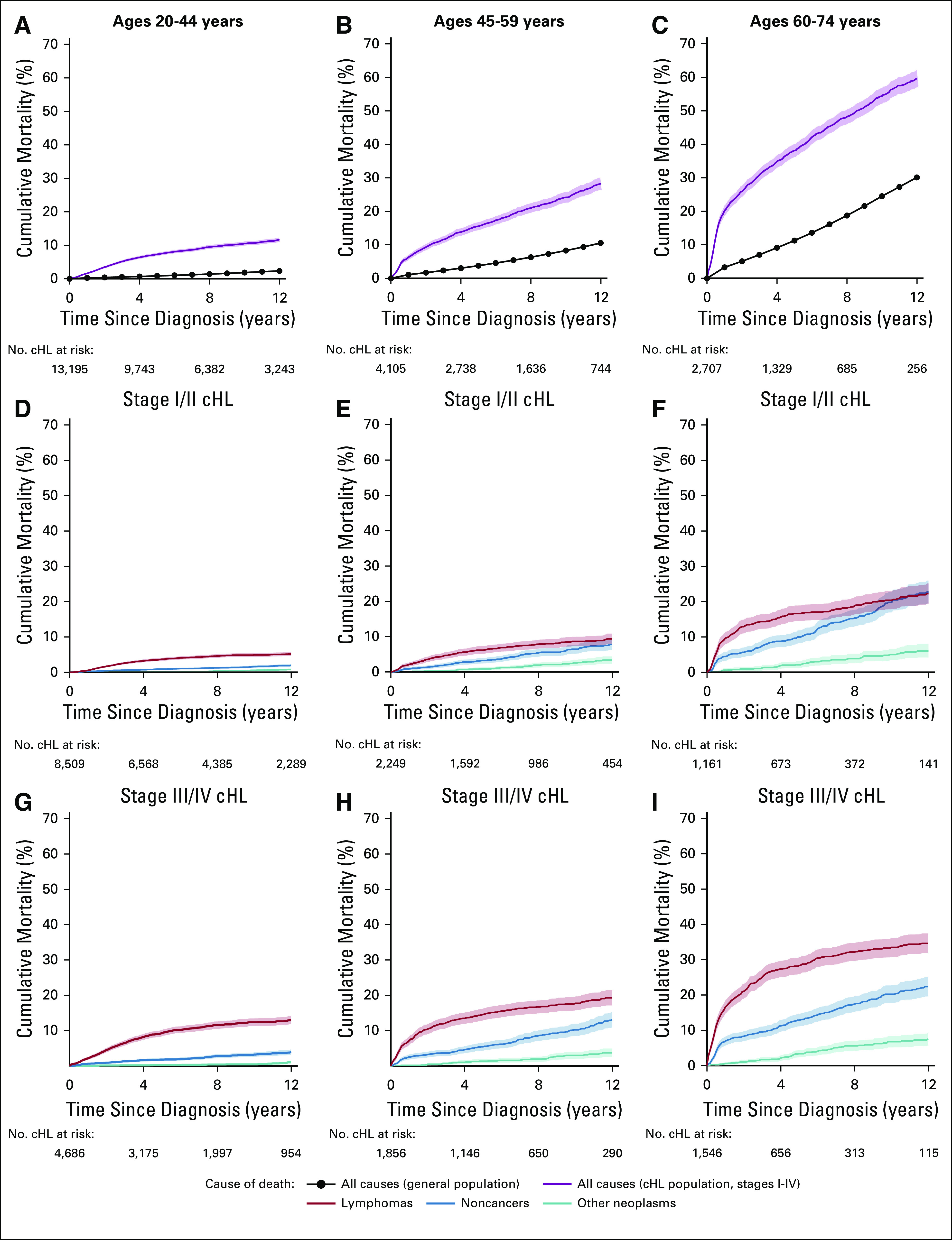
Results: We identified 3,380 deaths in the cHL cohort, including 1,321 (39%) not attributed to lymphoma. Overall, noncancer SMRs were increased 2.4-fold (95% CI, 2.2 to 2.6; observed, 559; EAR, 61.6) and 1.6-fold (95% CI, 1.4 to 1.7; observed, 473; EAR, 18.2) for advanced- and early-stage cHL, respectively, compared with the general US population. SMRs and EARs differed substantially by cause of death and cHL stage. Among the highest EARs for noncancer causes of death were those for heart disease (EAR, 15.1; SMR, 2.1), infections (EAR, 10.6; SMR, 3.9), interstitial lung disease (ILD; EAR, 9.7; SMR, 22.1), and adverse events (AEs) related to medications/drugs (EAR, 7.4; SMR, 5.0) after advanced-stage cHL and heart disease (EAR, 6.6; SMR, 1.7), ILD (EAR, 3.7; SMR, 13.1), and infections (EAR, 3.1; SMR, 2.2) after early-stage cHL. Strikingly elevated SMRs for ILD, infections, and AEs were observed < 1 year after cHL. Individuals age 60-74 years with advanced-stage cHL experienced a disproportionate excess of deaths as a result of heart disease, ILD, infections, AEs, and solid tumors.
Conclusion: Despite evolving cHL treatment approaches, patients continue to face increased nonlymphoma mortality risks from multiple, potentially preventable causes. Surveillance, early interventions, and cHL treatment refinements may favorably affect patient longevity, particularly among high-risk subgroups.
Figures
Comment in
-
Continuum of Care for Hodgkin Lymphoma: Impact of Modern Therapy on Postacute Morbidity and Mortality.J Clin Oncol. 2020 Dec 10;38(35):4131-4134. doi: 10.1200/JCO.20.02668. Epub 2020 Oct 8. J Clin Oncol. 2020. PMID: 33030980 Free PMC article. No abstract available.
References
-
- Aleman BM, van den Belt-Dusebout AW, Klokman WJ, et al. Long-term cause-specific mortality of patients treated for Hodgkin’s disease. J Clin Oncol. 2003;21:3431–3439. - PubMed
-
- Bhuller KS, Zhang Y, Li D, et al. Late mortality, secondary malignancy and hospitalisation in teenage and young adult survivors of Hodgkin lymphoma: Report of the Childhood/Adolescent/Young Adult Cancer Survivors Research Program and the BC Cancer Agency Centre for Lymphoid Cancer. Br J Haematol. 2016;172:757–768. - PubMed
-
- Kero AE, Järvelä LS, Arola M, et al. Late mortality among 5-year survivors of early onset cancer: A population-based register study. Int J Cancer. 2015;136:1655–1664. - PubMed
-
- Ng AK, Bernardo MP, Weller E, et al. Long-term survival and competing causes of death in patients with early-stage Hodgkin’s disease treated at age 50 or younger. J Clin Oncol. 2002;20:2101–2108. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
