

Longer Follow-Up Confirms Recurrence-Free Survival Benefit of Adjuvant Pembrolizumab in High-Risk Stage III Melanoma: Updated Results From the EORTC 1325-MG/KEYNOTE-054 Trial
- PMID: 32946353
- PMCID: PMC7676886
- DOI: 10.1200/JCO.20.02110
Longer Follow-Up Confirms Recurrence-Free Survival Benefit of Adjuvant Pembrolizumab in High-Risk Stage III Melanoma: Updated Results From the EORTC 1325-MG/KEYNOTE-054 Trial
Abstract
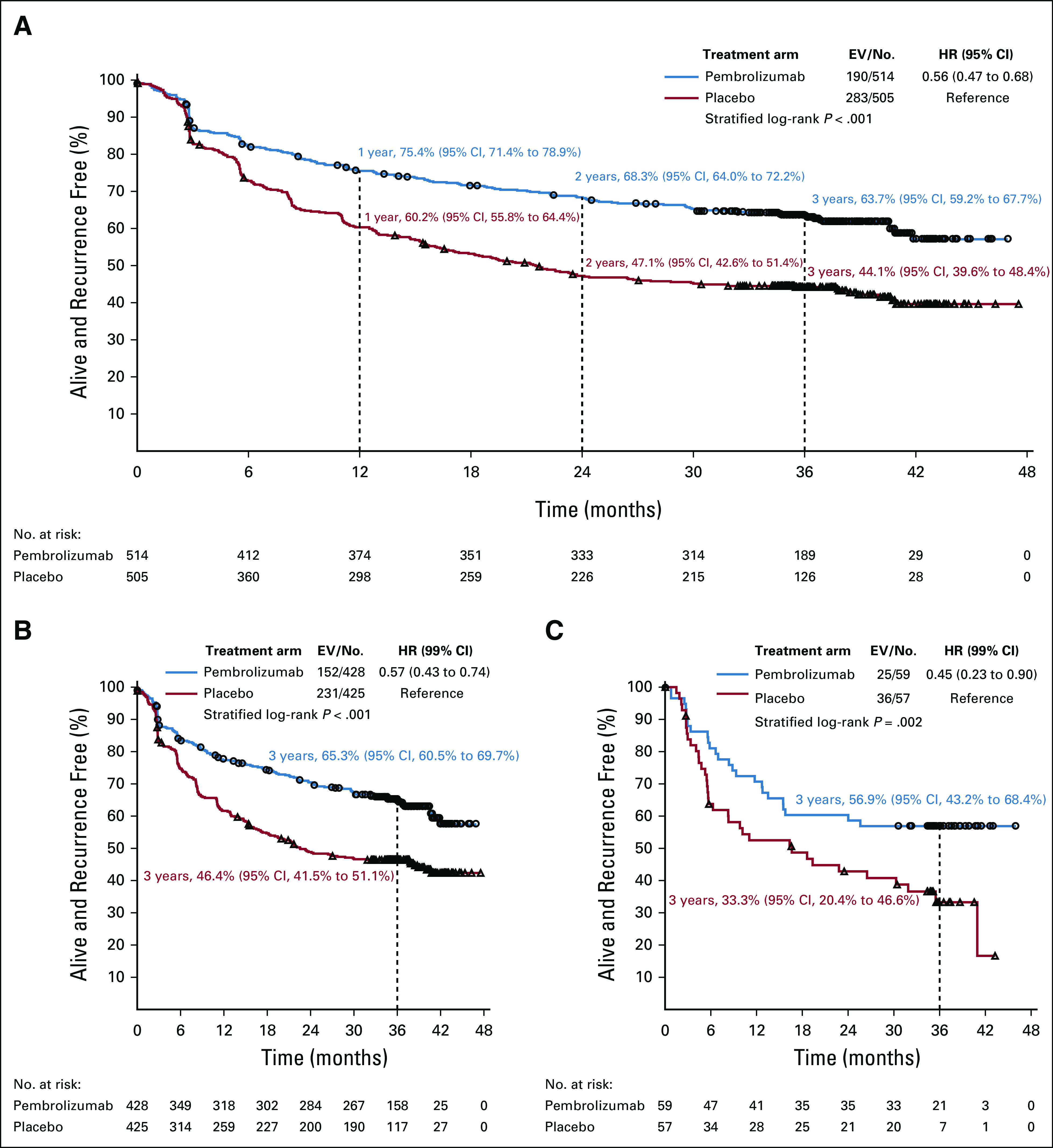
Purpose: We conducted the phase III double-blind European Organisation for Research and Treatment of Cancer (EORTC) 1325/KEYNOTE-054 trial to evaluate pembrolizumab versus placebo in patients with resected high-risk stage III melanoma. On the basis of 351 recurrence-free survival (RFS) events at a 1.25-year median follow-up, pembrolizumab prolonged RFS (hazard ratio [HR], 0.57; P < .0001) compared with placebo. This led to the approval of pembrolizumab adjuvant treatment by the European Medicines Agency and US Food and Drug Administration. Here, we report an updated RFS analysis at the 3.05-year median follow-up.
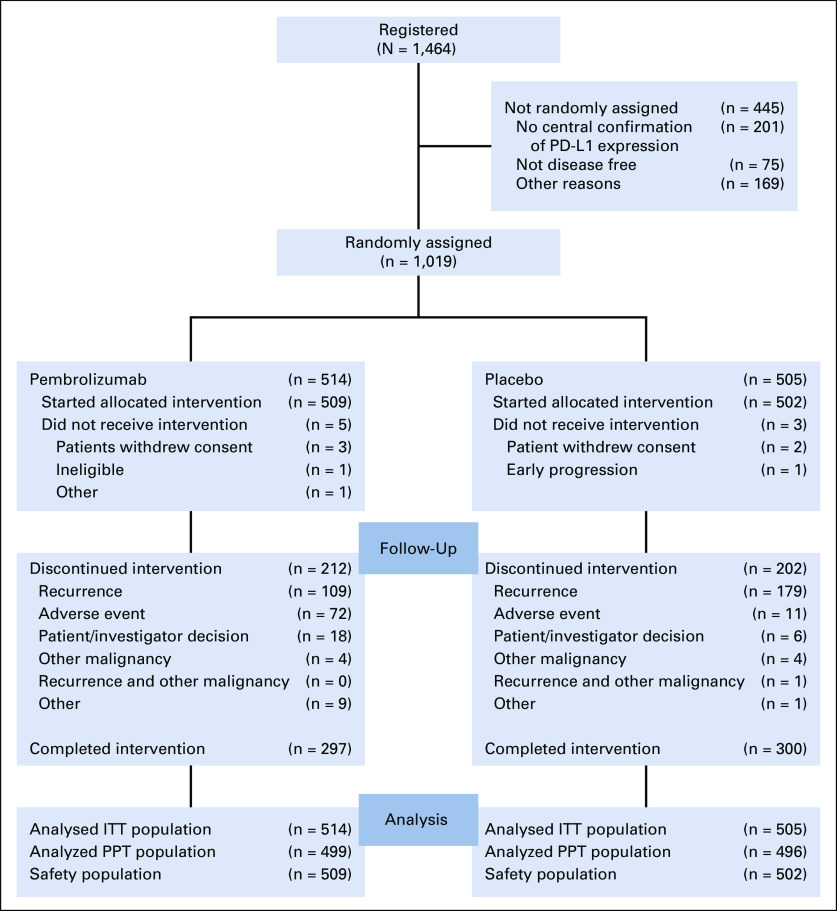
Patients and methods: A total of 1,019 patients with complete lymph node dissection of American Joint Committee on Cancer Staging Manual (seventh edition; AJCC-7), stage IIIA (at least one lymph node metastasis > 1 mm), IIIB, or IIIC (without in-transit metastasis) cutaneous melanoma were randomly assigned to receive pembrolizumab at a flat dose of 200 mg (n = 514) or placebo (n = 505) every 3 weeks for 1 year or until disease recurrence or unacceptable toxicity. The two coprimary end points were RFS in the overall population and in those with programmed death-ligand 1 (PD-L1)-positive tumors.
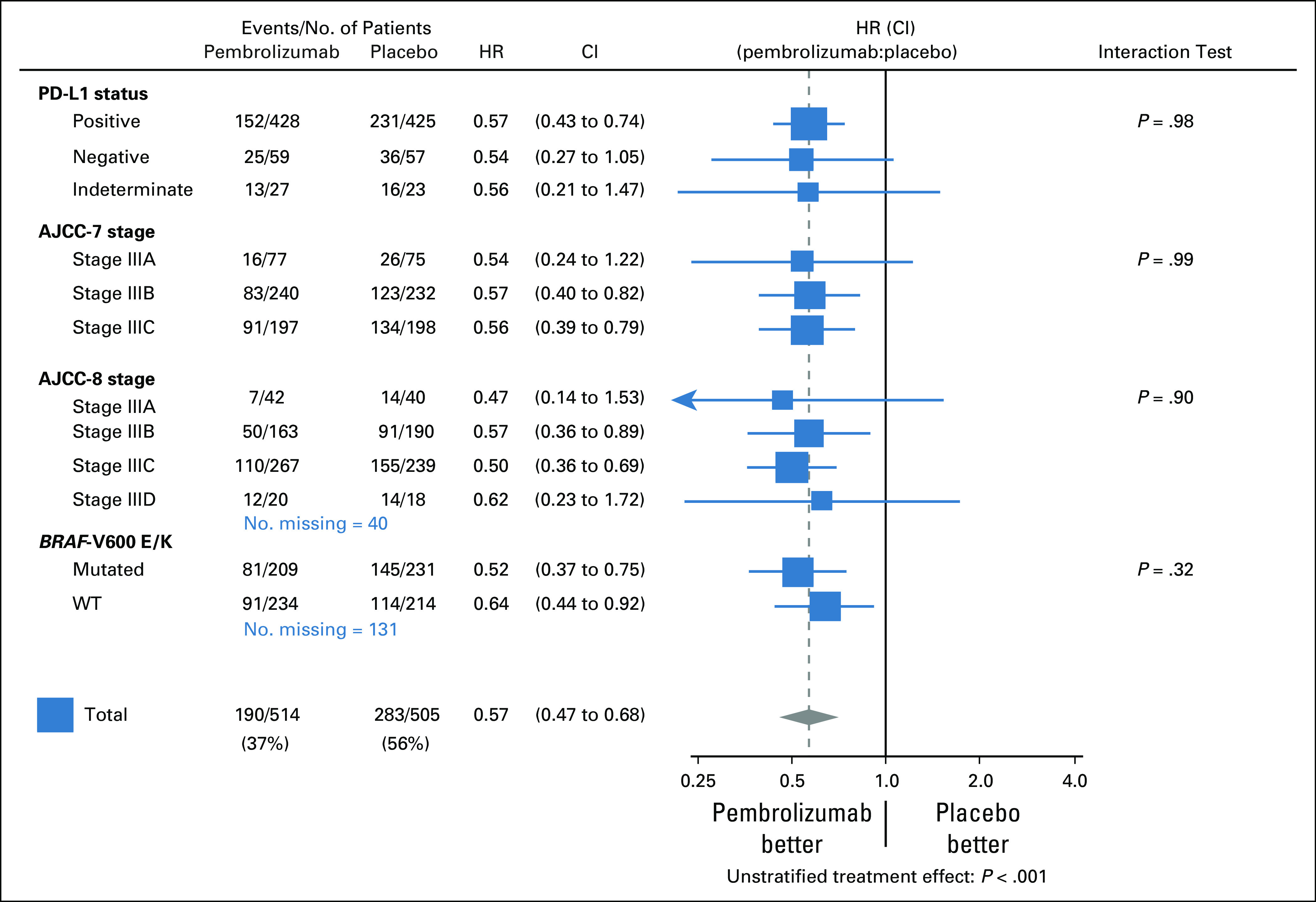
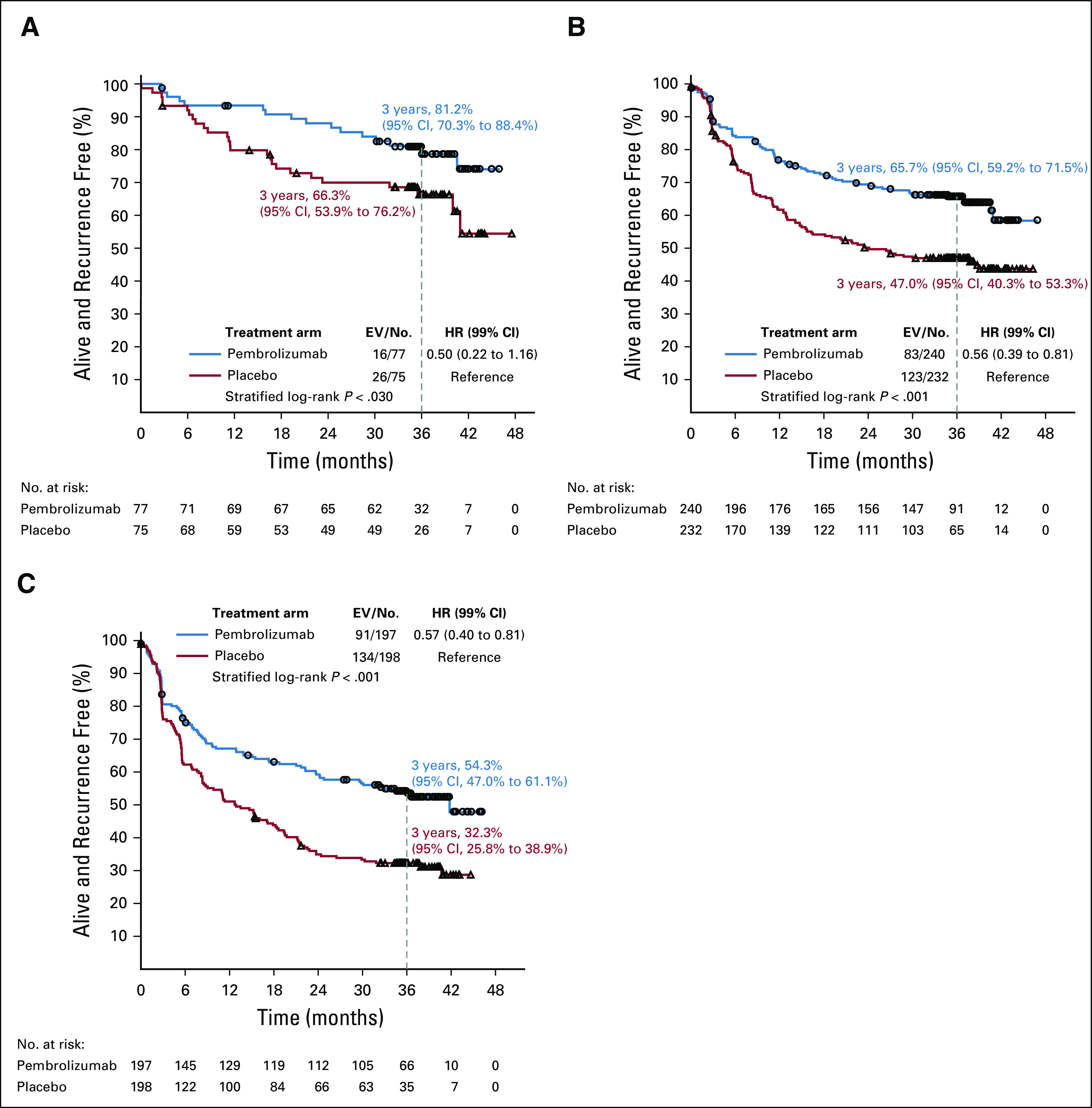
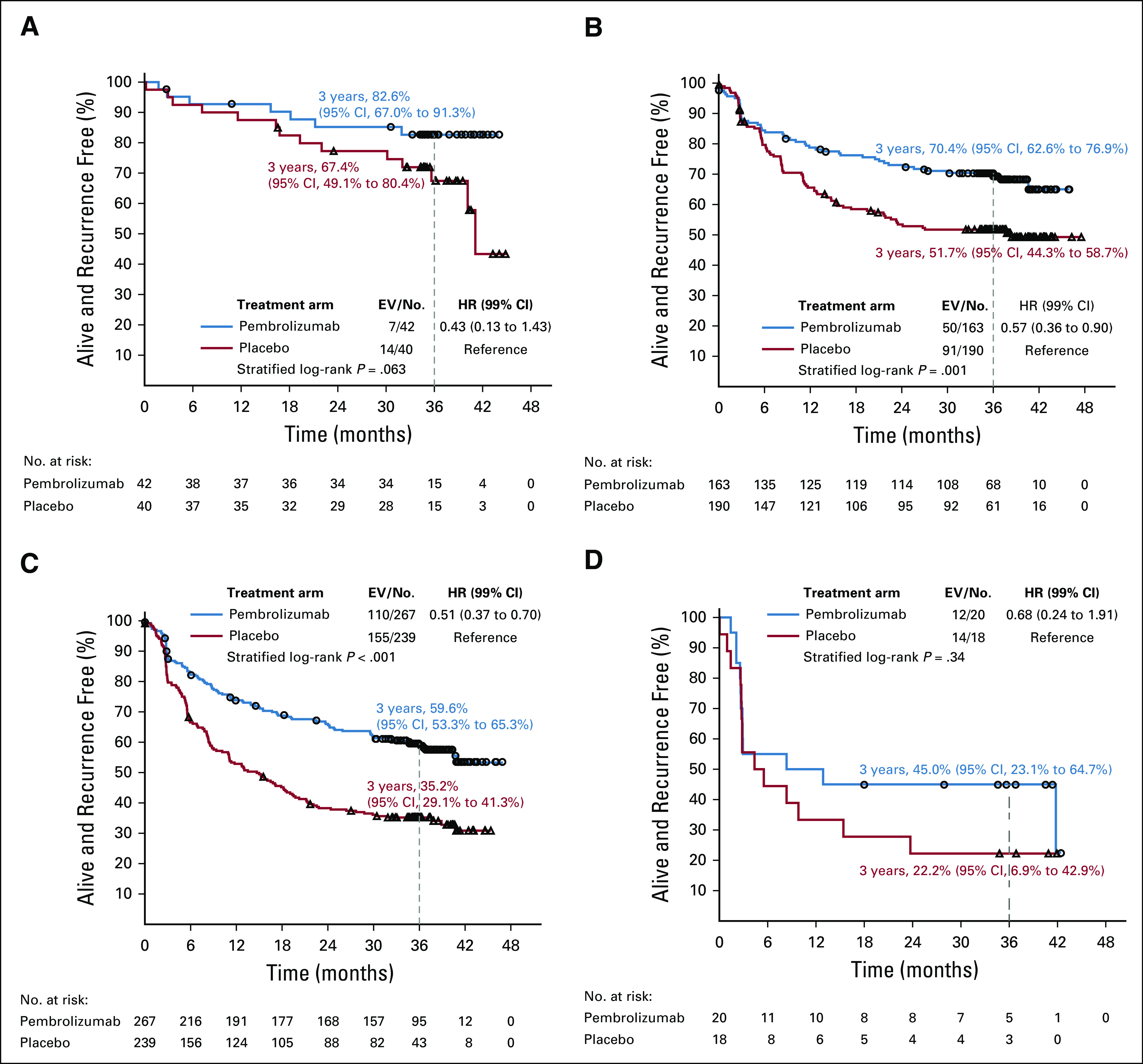
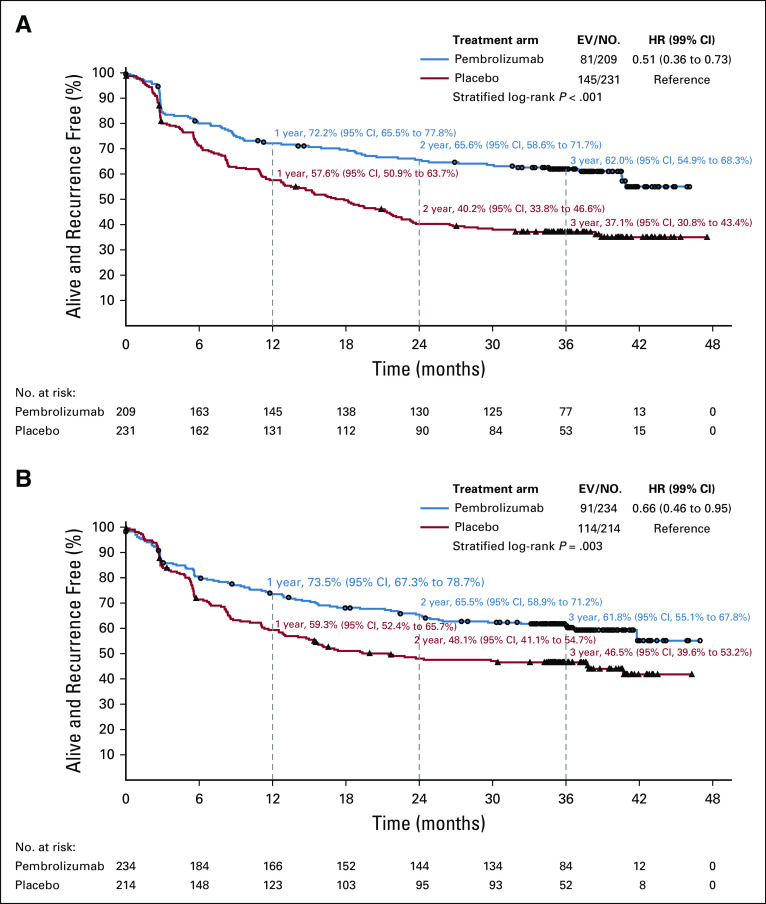
Results: Pembrolizumab (190 RFS events) compared with placebo (283 RFS events) resulted in prolonged RFS in the overall population (3-year RFS rate, 63.7% v 44.1% for pembrolizumab v placebo, respectively; HR, 0.56; 95% CI, 0.47 to 0.68) and in the PD-L1-positive tumor subgroup (HR, 0.57; 99% CI, 0.43 to 0.74). The impact of pembrolizumab on RFS was similar in subgroups, in particular according to AJCC-7 and AJCC-8 staging, and BRAF mutation status (HR, 0.51 [99% CI, 0.36 to 0.73] v 0.66 [99% CI, 0.46 to 0.95] for V600E/K v wild type).
Conclusion: In resected high-risk stage III melanoma, pembrolizumab adjuvant therapy provided a sustained and clinically meaningful improvement in RFS at 3-year median follow-up. This improvement was consistent across subgroups.
Trial registration: ClinicalTrials.gov NCT02362594.
Figures
Comment in
-
Considerations on the Role of Pembrolizumab Adjuvant Therapy in AJCC-8 Stage IIIA Melanoma.J Clin Oncol. 2021 Mar 10;39(8):943-944. doi: 10.1200/JCO.20.03213. Epub 2021 Jan 25. J Clin Oncol. 2021. PMID: 33492983 No abstract available.
-
Reply to E. Hindié.J Clin Oncol. 2021 Mar 10;39(8):944-946. doi: 10.1200/JCO.20.03463. Epub 2021 Jan 25. J Clin Oncol. 2021. PMID: 33492998 No abstract available.
References
-
- Eggermont AMM, Spatz A, Robert C: Cutaneous melanoma. Lancet 383:816-827, 2014 - PubMed
-
- Ugurel S Röhmel J Ascierto PA, et al. : Survival of patients with advanced metastatic melanoma: The impact of MAP kinase pathway inhibition and immune checkpoint inhibition - Update 2019. Eur J Cancer 130:126-138, 2020 - PubMed
-
- Eggermont AM Chiarion-Sileni V Grob JJ, et al. : Adjuvant ipilimumab versus placebo after complete resection of high-risk stage III melanoma (EORTC 18071): A randomised, double-blind, phase 3 trial. Lancet Oncol 16:522-530, 2015 - PubMed
-
- Eggermont AMM Chiarion-Sileni V Grob JJ, et al. : Adjuvant ipilimumab versus placebo after complete resection of stage III melanoma: Long-term follow-up results of the European Organisation for Research and Treatment of Cancer 18071 double-blind phase 3 randomised trial. Eur J Cancer 119:1-10, 2019 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
